2. SARS-CoV-2 Virus
2.1. Structure of the SARS-CoV-2 Spike Glycoprotein
The SARS-CoV-2, a β-coronavirus, exhibits a complex viral architecture characterized by spike proteins (S) organized in trimers on its surface. These proteins play a pivotal role in the infection process, divided into two functional subunits: S1 and S2. The S1 subunit specifically recognizes angiotensin-converting enzyme 2 (ACE2), expressed on the surface of various human organs. This interaction initiates viral entry into the host. Once bound to ACE2, the S2 subunit of the spike protein facilitates fusion of the virus with the host cell membrane, thereby releasing its viral genetic material into the host cell.
The sophisticated structure of the SARS-CoV-2 spike protein, characterized by its high affinity for ACE2 and the presence of a furin cleavage site, distinguishes it from other coronaviruses. This specific interaction with ACE2 is particularly significant in the respiratory tract, heart, kidneys, and other organs where ACE2 is expressed. This specificity enhances the virus's infectivity and pathogenicity in infected individuals.
By utilizing ACE2 as a key receptor, SARS-CoV-2 evades cellular defenses and exploits normal cellular processes for its entry and replication, thereby facilitating rapid spread of infection. Understanding the intricate structure and function of these mechanisms is crucial for guiding the development of targeted therapeutic and vaccine strategies against SARS-CoV-2.
| [4] | Walls AC, Park YJ, Tortorici MA, Wall A, McGuire AT, Veesler D. Structure, Function, and Antigenicity of the SARS-CoV-2 Spike Glycoprotein. Cell. 2020; 181(2): 281-292. e6. https://doi.org/10.1016/j.cell.2020.02.058 |
| [5] | Wrapp D, Wang N, Corbett KS, Goldsmith JA, Hsieh CL, Abiona O, Graham BS, McLellan JS. Cryo-EM structure of the 2019-nCoV spike in the prefusion conformation. Science. 2020; 367(6483): 1260-1263. https://doi.org/10.1126/science.abb2507 |
| [6] | Hoffmann M, Kleine-Weber H, Schroeder S, Krüger N, Herrler T, Erichsen S, Schiergens TS, Herrler G, Wu NH, Nitsche A, Müller MA, Drosten C, Pöhlmann S. SARS-CoV-2 Cell Entry Depends on ACE2 and TMPRSS2 and Is Blocked by a Clinically Proven Protease Inhibitor. Cell. 2020; 181(2): 271-280. e8. https://doi.org/10.1016/j.cell.2020.02.052 |
[4-6]
2.2. Molecular Architecture of the SARS-CoV-2
SARS-CoV-2 utilizes its spike protein (S protein) to infect host cells. This protein consists of two primary subunits, S1 and S2, with S1 containing the receptor-binding domain (RBD) crucial for specific interaction with angiotensin-converting enzyme 2 (ACE2) on human cell surfaces. Initially adopting a 'down' conformation with approximately 10 glycans, the RBD structure is susceptible to modification through glycosylation processes. Upon binding to ACE2, a significant conformational change occurs, termed 'RBD up,' enhancing its interaction with ACE2.
Binding of RBD to ACE2 can also activate proteolytic cleavage of the S protein by proteases like furin, between subunits S1 and S2. This cleavage exposes subunit S2, essential for fusion with the host cell membrane, thereby facilitating viral RNA entry into the host cell to initiate infection.
To ensure its infectious efficacy, SARS-CoV-2 must efficiently package its 30 kb RNA within a confined space of approximately 80 nm in virion diameter. Observations suggest that ribonucleoproteins (RNPs), consisting of viral RNA and viral proteins like nucleocapsid proteins (N-proteins), are densely packed within the viral lumen. This densely packed and sometimes locally ordered arrangement of RNPs minimizes RNA entanglement and potential damage, optimizing packaging efficiency and ensuring viral genomic stability.
Cryo-ET and SDS-PAGE/MS analysis indicates that these densities likely represent RNPs, aligned using spherical masks revealing bucket-like and reverse G-shaped architectures with specific dimensions. These structures are crucial for fusion with the host cell membrane and viral infection initiation, closely associated with the viral envelope, forming assemblies in 'hexagon' or 'pyramid' shapes depending on the virion's geometry.
| [4] | Walls AC, Park YJ, Tortorici MA, Wall A, McGuire AT, Veesler D. Structure, Function, and Antigenicity of the SARS-CoV-2 Spike Glycoprotein. Cell. 2020; 181(2): 281-292. e6. https://doi.org/10.1016/j.cell.2020.02.058 |
| [9] | Zhu N, Wang W, Liu Z, et al. Morphogenesis and cytopathic effect of SARS-CoV-2 infection in human airway epithelial cells. Nature Communications. 2020; 11: 3910. https://doi.org/10.1038/s41467-020-17796-z |
[4, 9]
In summary, this study underscores the pivotal role of RNPs in viral assembly, enhancing the virus's resilience against environmental and physical challenges. However, precise mechanisms governing RNP assembly and their interaction with other viral components remain to be fully elucidated.
| [5] | Wrapp D, Wang N, Corbett KS, Goldsmith JA, Hsieh CL, Abiona O, Graham BS, McLellan JS. Cryo-EM structure of the 2019-nCoV spike in the prefusion conformation. Science. 2020; 367(6483): 1260-1263. https://doi.org/10.1126/science.abb2507 |
| [6] | Hoffmann M, Kleine-Weber H, Schroeder S, Krüger N, Herrler T, Erichsen S, Schiergens TS, Herrler G, Wu NH, Nitsche A, Müller MA, Drosten C, Pöhlmann S. SARS-CoV-2 Cell Entry Depends on ACE2 and TMPRSS2 and Is Blocked by a Clinically Proven Protease Inhibitor. Cell. 2020; 181(2): 271-280. e8. https://doi.org/10.1016/j.cell.2020.02.052 |
[5, 6]
2.3. Cryo-EM structure of the SRAS-COV-2 in the Prefusion Conformation
Operating at a resolution of 3.5 angstroms, cryo-electron microscopy delineates an "open" trimeric conformation of the receptor-binding domain (RBD), underscoring its accessibility for receptor binding and subsequent viral invasion. Notably, this crystallographic analysis highlights a robust affinity of approximately 15 nM between the Spike protein of SARS-CoV-2 and ACE2, surpassing that observed with related coronaviruses like SARS-CoV, thereby elucidating the heightened transmissibility observed with SARS-CoV-2 in human populations.
| [4] | Walls AC, Park YJ, Tortorici MA, Wall A, McGuire AT, Veesler D. Structure, Function, and Antigenicity of the SARS-CoV-2 Spike Glycoprotein. Cell. 2020; 181(2): 281-292. e6. https://doi.org/10.1016/j.cell.2020.02.058 |
| [10] | Yan R, Zhang Y, Li Y, et al. Structural basis for the recognition of SARS-CoV-2 by full-length human ACE2. Science. 2020; 367(6485): 1444-1448. https://doi.org/10.1126/science.abb2762 |
[4, 10]
The detailed cryo-electron microscopy analysis of the Spike protein (S) from SARS-CoV-2 in its prefusion conformation reveals critical insights into its intricate architecture and functional mechanisms. As a class I trimeric fusion protein, Spike (S) undergoes substantial structural rearrangements in its metastable state to facilitate viral entry into host cells. Comprising two functional subunits, S1 and S2, the former harbors the receptor-binding domain (RBD) specific to angiotensin-converting enzyme 2 (ACE2), pivotal on the surface of host cells.
| [4] | Walls AC, Park YJ, Tortorici MA, Wall A, McGuire AT, Veesler D. Structure, Function, and Antigenicity of the SARS-CoV-2 Spike Glycoprotein. Cell. 2020; 181(2): 281-292. e6. https://doi.org/10.1016/j.cell.2020.02.058 |
| [10] | Yan R, Zhang Y, Li Y, et al. Structural basis for the recognition of SARS-CoV-2 by full-length human ACE2. Science. 2020; 367(6485): 1444-1448. https://doi.org/10.1126/science.abb2762 |
[4, 10]
Upon encountering a human cell, the RBD of S1 binds ACE2 with high specificity, triggering a conformational shift within the Spike protein. Initially nestled in a "down" position against the protein, the RBD transitions to an "up" conformation, thereby exposing its binding epitope and optimizing interaction with ACE2. This structural alteration enhances the efficiency of viral entry into the host cell.
Once engaged with ACE2, the S2 subunit of the Spike protein facilitates membrane fusion between the viral envelope and the cellular membrane. This fusion event enables the release of viral genetic material into the host cell, initiating the viral replication cycle.
| [4] | Walls AC, Park YJ, Tortorici MA, Wall A, McGuire AT, Veesler D. Structure, Function, and Antigenicity of the SARS-CoV-2 Spike Glycoprotein. Cell. 2020; 181(2): 281-292. e6. https://doi.org/10.1016/j.cell.2020.02.058 |
| [10] | Yan R, Zhang Y, Li Y, et al. Structural basis for the recognition of SARS-CoV-2 by full-length human ACE2. Science. 2020; 367(6485): 1444-1448. https://doi.org/10.1126/science.abb2762 |
[4, 10]
2.4. Structural Basis for the Recognition of SARS-CoV-2 by Full-Length Human ACE2
The recognition of SARS-CoV-2 by full-length human ACE2 involves intricate molecular interactions that govern viral entry and infectivity. SARS-CoV-2, a novel coronavirus that emerged in late 2019, utilizes its spike protein (S) to bind to the human ACE2 receptor on host cells, thereby facilitating viral entry and subsequent infection. Understanding the detailed molecular interactions between the viral S protein and ACE2 receptor is crucial for elucidating COVID-19 pathogenesis and developing effective therapeutic strategies.
The spike protein of SARS-CoV-2 consists of two functional subunits: S1, responsible for receptor binding, and S2, facilitating membrane fusion. Within the S1 subunit, the receptor-binding domain (RBD) specifically interacts with ACE2 on the host cell surface. High-resolution structural studies, including X-ray crystallography and cryo-electron microscopy, have provided key insights into this interaction. The RBD of the SARS-CoV-2 spike protein adopts a conformation that optimally binds to ACE2, similar to its predecessor SARS-CoV, despite distinct sequence variations.
Structural analyses have highlighted critical amino acid residues in both the spike protein RBD and ACE2 receptor that govern their affinity and specificity. Notably, amino acid residues such as lysine 31 and glutamine 42 on ACE2 form hydrogen bonds with residues on the RBD, enhancing binding affinity. This interaction induces a conformational change in the spike protein, facilitating membrane fusion and viral entry into the host cell. Insights from these structural studies not only deepen our understanding of viral entry mechanisms but also provide a foundation for developing targeted therapies, including neutralizing antibodies and small molecule inhibitors, aimed at disrupting the SARS-CoV-2-ACE2 interaction to effectively combat COVID-19.
| [4] | Walls AC, Park YJ, Tortorici MA, Wall A, McGuire AT, Veesler D. Structure, Function, and Antigenicity of the SARS-CoV-2 Spike Glycoprotein. Cell. 2020; 181(2): 281-292. e6. https://doi.org/10.1016/j.cell.2020.02.058 |
| [10] | Yan R, Zhang Y, Li Y, et al. Structural basis for the recognition of SARS-CoV-2 by full-length human ACE2. Science. 2020; 367(6485): 1444-1448. https://doi.org/10.1126/science.abb2762 |
[4, 10]
2.5. The Mechanism of SARS-CoV-2 Entry
The SARS-CoV-2 virus, responsible for the global COVID-19 pandemic since 2020, belongs to the Betacoronavirus family and shares significant similarity with the SARS-CoV virus that caused the 2002-2004 SARS outbreak.
This enveloped, single-stranded RNA virus utilizes the angiotensin-converting enzyme 2 (ACE2) as its cellular receptor, a mechanism also exploited by other coronaviruses like HCoV-NL63 and MERS-CoV. The viral structure includes nucleocapsid (N), membrane (M), envelope (E), and spike (S) proteins, with the S protein being crucial for membrane fusion. The S protein, cleaved into S1 (for ACE2 binding) and S2 (for membrane fusion) subunits by proprotein convertases like furin, plays a vital role in the infection process. Viral infection induces the formation of perinuclear membrane-bound replication organelles likely derived from the endoplasmic reticulum, where viral replication and virion assembly occur. Upon assembly, virions are transported to the ER-Golgi intermediate compartment for final maturation and release.
| [4] | Walls AC, Park YJ, Tortorici MA, Wall A, McGuire AT, Veesler D. Structure, Function, and Antigenicity of the SARS-CoV-2 Spike Glycoprotein. Cell. 2020; 181(2): 281-292. e6. https://doi.org/10.1016/j.cell.2020.02.058 |
| [11] | Shang J, Ye G, Shi K, et al. Structural basis of receptor recognition by SARS-CoV-2. Nature. 2020; 581(7807): 221-224. https://doi.org/10.1038/s41586-020-2179-x |
[4, 11]
The conformational changes induced by the S protein's interaction with ACE2 enable membrane fusion, facilitating the entry of viral genome into the host cell. The three-dimensional structure of the S protein, revealed through cryo-electron microscopy studies, provides crucial insights into its pre- and post-fusion conformations, particularly its receptor-binding domain (RBD), the primary site of interaction with ACE2 and a major target for neutralizing antibodies. The Spike protein (S) of SARS-CoV-2 plays a central role in viral infection by interacting with the ACE2 receptor on human cells. Comprising predominantly β-sheet structured C-terminal domains, the protein includes the critical receptor-binding domain (RBD).
This RBD facilitates virus attachment by linking the CTD1 and CTD2 domains of the Spike protein, essential for virus fusion with the cell membrane. In its prefusion form, the S2 subunit of the protein adopts a three-stranded coil conformation critical for structural stability. After fusion, this subunit reorganizes into a rigid six-helix bundle, promoting virus insertion into the host cell. ACE2, the receptor for SARS-CoV-2, is an enzyme primarily present in respiratory pathways but also in other tissues like the colon and kidneys.
| [4] | Walls AC, Park YJ, Tortorici MA, Wall A, McGuire AT, Veesler D. Structure, Function, and Antigenicity of the SARS-CoV-2 Spike Glycoprotein. Cell. 2020; 181(2): 281-292. e6. https://doi.org/10.1016/j.cell.2020.02.058 |
| [10] | Yan R, Zhang Y, Li Y, et al. Structural basis for the recognition of SARS-CoV-2 by full-length human ACE2. Science. 2020; 367(6485): 1444-1448. https://doi.org/10.1126/science.abb2762 |
[4, 10]
The interaction between the Spike protein's RBD and ACE2 is crucial for viral entry into human cells, influencing the virus's ability to infect and spread within the body. ACE2 expression varies across tissues and can be modulated by factors such as age, sex, and medical conditions like hypertension and diabetes, potentially affecting COVID-19 severity in infected individuals.
| [4] | Walls AC, Park YJ, Tortorici MA, Wall A, McGuire AT, Veesler D. Structure, Function, and Antigenicity of the SARS-CoV-2 Spike Glycoprotein. Cell. 2020; 181(2): 281-292. e6. https://doi.org/10.1016/j.cell.2020.02.058 |
| [11] | Shang J, Ye G, Shi K, et al. Structural basis of receptor recognition by SARS-CoV-2. Nature. 2020; 581(7807): 221-224. https://doi.org/10.1038/s41586-020-2179-x |
[4, 11]
2.6. The Immune Response to SARS-CoV-2 and Mechanisms of Immunopathological Changes in COVID-19
2.6.1. The Structure of the SARS-CoV-2
SARS-CoV-2, the virus responsible for the global COVID-19 pandemic that began in 2020, belongs to the Betacoronavirus family and shares significant similarity with SARS-CoV, the agent of the 2002-2004 SARS outbreak. This enveloped, single-stranded RNA virus uses angiotensin-converting enzyme 2 (ACE2) as its cellular receptor, a mechanism also employed by other coronaviruses such as HCoV-NL63 and MERS-CoV.
| [6] | Hoffmann M, Kleine-Weber H, Schroeder S, Krüger N, Herrler T, Erichsen S, Schiergens TS, Herrler G, Wu NH, Nitsche A, Müller MA, Drosten C, Pöhlmann S. SARS-CoV-2 Cell Entry Depends on ACE2 and TMPRSS2 and Is Blocked by a Clinically Proven Protease Inhibitor. Cell. 2020; 181(2): 271-280. e8. https://doi.org/10.1016/j.cell.2020.02.052 |
| [12] | Zhou P, Yang XL, Wang XG, et al. A pneumonia outbreak associated with a new coronavirus of probable bat origin. Nature. 2020; 579(7798): 270-273. https://doi.org/10.1038/s41586-020-2012-7 |
| [13] | Letko M, Marzi A, Munster V. Functional assessment of cell entry and receptor usage for SARS-CoV-2 and other lineage B betacoronaviruses. Nature Microbiology. 2020; 5(4): 562-569. https://doi.org/10.1038/s41564-020-0688-y |
[6, 12, 13]
The viral structure comprises nucleocapsid (N), membrane (M), envelope (E), and spike (S) proteins, with the spike protein being crucial for membrane fusion with the host cell. The spike protein is cleaved into S1 (responsible for ACE2 binding) and S2 (responsible for membrane fusion) subunits by proprotein convertases like furin, playing an essential role in the infection process. Infection by the virus induces the formation of perinuclear replication organelles derived likely from the endoplasmic reticulum, where viral replication and virion assembly occur. Once assembled, the virions are transported to the ER-Golgi intermediate compartment for final maturation and release.
The conformational changes induced by the interaction of the spike protein with ACE2 allow membrane fusion, facilitating the entry of the viral genome into the host cell. The three-dimensional structure of the spike protein, determined by cryo-electron microscopy studies, reveals crucial details about its pre- and post-fusion conformation and its receptor-binding domain (RBD), the main site of interaction with ACE2 and a major target for neutralizing antibodies.
| [6] | Hoffmann M, Kleine-Weber H, Schroeder S, Krüger N, Herrler T, Erichsen S, Schiergens TS, Herrler G, Wu NH, Nitsche A, Müller MA, Drosten C, Pöhlmann S. SARS-CoV-2 Cell Entry Depends on ACE2 and TMPRSS2 and Is Blocked by a Clinically Proven Protease Inhibitor. Cell. 2020; 181(2): 271-280. e8. https://doi.org/10.1016/j.cell.2020.02.052 |
| [12] | Zhou P, Yang XL, Wang XG, et al. A pneumonia outbreak associated with a new coronavirus of probable bat origin. Nature. 2020; 579(7798): 270-273. https://doi.org/10.1038/s41586-020-2012-7 |
| [13] | Letko M, Marzi A, Munster V. Functional assessment of cell entry and receptor usage for SARS-CoV-2 and other lineage B betacoronaviruses. Nature Microbiology. 2020; 5(4): 562-569. https://doi.org/10.1038/s41564-020-0688-y |
[6, 12, 13]
2.6.2. Structure of the SARS-CoV-2 Spike Glycoprotein
The spike protein (S) of SARS-CoV-2 plays a central role in viral infection by interacting with the ACE2 receptor on human cells. Composed mainly of β-sheet structured C-terminal domains, the spike protein includes the crucial receptor-binding domain (RBD).
This RBD facilitates viral attachment by linking the CTD1 and CTD2 domains of the spike protein, essential for viral fusion with the cellular membrane. In its prefusion form, the S2 subunit of the spike protein adopts a three-stranded coil configuration crucial for structural stability. Post-fusion, this subunit rearranges into a rigid six-helix structure, promoting the insertion of the virus into the host cell.
| [6] | Hoffmann M, Kleine-Weber H, Schroeder S, Krüger N, Herrler T, Erichsen S, Schiergens TS, Herrler G, Wu NH, Nitsche A, Müller MA, Drosten C, Pöhlmann S. SARS-CoV-2 Cell Entry Depends on ACE2 and TMPRSS2 and Is Blocked by a Clinically Proven Protease Inhibitor. Cell. 2020; 181(2): 271-280. e8. https://doi.org/10.1016/j.cell.2020.02.052 |
| [12] | Zhou P, Yang XL, Wang XG, et al. A pneumonia outbreak associated with a new coronavirus of probable bat origin. Nature. 2020; 579(7798): 270-273. https://doi.org/10.1038/s41586-020-2012-7 |
| [13] | Letko M, Marzi A, Munster V. Functional assessment of cell entry and receptor usage for SARS-CoV-2 and other lineage B betacoronaviruses. Nature Microbiology. 2020; 5(4): 562-569. https://doi.org/10.1038/s41564-020-0688-y |
[6, 12, 13]
ACE2, the receptor for SARS-CoV-2, is an enzyme present primarily in the respiratory tract but also in other tissues like the colon and kidneys. The interaction between the RBD of the spike protein and ACE2 is crucial for viral entry into human cells, influencing the virus's ability to infect and spread within the body. ACE2 expression varies across tissues and can be modulated by factors such as age, sex, and medical conditions like hypertension and diabetes, which may play a role in the severity of COVID-19 in infected individuals.
| [4] | Walls AC, Park YJ, Tortorici MA, Wall A, McGuire AT, Veesler D. Structure, Function, and Antigenicity of the SARS-CoV-2 Spike Glycoprotein. Cell. 2020; 181(2): 281-292. e6. https://doi.org/10.1016/j.cell.2020.02.058 |
[4]
2.6.3. The Mechanism of SARS-CoV-2 Entry
SARS-CoV-2 employs two primary pathways for host cell entry: the cell surface-dependent pathway and the endosomal pathway. In the cell surface-dependent pathway, the virus's spike protein undergoes cleavage by furin within virus-producing cells and subsequently by the host cell surface enzyme TMPRSS2. This process exposes the fusion peptide, facilitating direct fusion with the host cell membrane and the release of viral RNA into the cytoplasm. In the endosomal pathway, the virus is internalized via endocytosis and enclosed within an endosome. Here, the spike protein is cleaved by cathepsin L, also exposing the fusion peptide and releasing viral RNA into the cytoplasm. ACE2 expression varies across tissues, influencing viral tropism and disease severity. Comorbidities such as asthma, obesity, and specific genetic conditions may modulate ACE2 expression, potentially impacting COVID-19 outcomes.
| [14] | Mehta P, McAuley DF, Brown M, Sanchez E, Tattersall RS, Manson JJ. COVID-19: consider cytokine storm syndromes and immunosuppression. The Lancet. 2020; 395(10229): 1033-1034. https://doi.org/10.1016/S0140-6736(20)30628-0 |
| [15] | Zhang C, Wu Z, Li JW, Zhao H, Wang GQ. The cytokine release syndrome (CRS) of severe COVID-19 and interleukin-6 receptor (IL-6R) antagonist Tocilizumab may be the key to reduce the mortality. International Journal of Antimicrobial Agents. 2020; 55(5): 105954. https://doi.org/10.1016/j.ijantimicag.2020.105954 PubMed. |
[14, 15]
The virus can adapt to different ACE2 variants, potentially originating from animal reservoirs like Rhinolophus bats via intermediate hosts such as civets. The severity of infection can vary based on these viral adaptations. Beyond ACE2, molecules like lectins (DC-SIGN and L-SIGN), TIM1, AXL, and CD147 are potential alternative receptors, yet their precise roles in SARS-CoV-2 infection require further investigation in medical research.
| [14] | Mehta P, McAuley DF, Brown M, Sanchez E, Tattersall RS, Manson JJ. COVID-19: consider cytokine storm syndromes and immunosuppression. The Lancet. 2020; 395(10229): 1033-1034. https://doi.org/10.1016/S0140-6736(20)30628-0 |
| [15] | Zhang C, Wu Z, Li JW, Zhao H, Wang GQ. The cytokine release syndrome (CRS) of severe COVID-19 and interleukin-6 receptor (IL-6R) antagonist Tocilizumab may be the key to reduce the mortality. International Journal of Antimicrobial Agents. 2020; 55(5): 105954. https://doi.org/10.1016/j.ijantimicag.2020.105954 PubMed. |
[14, 15]
The viral entry process of SARS-CoV-2 into host cells involves several crucial steps. Initially, the viral spike protein interacts with the cellular ACE2 receptor, facilitating membrane fusion. This interaction can be aided by the cell surface protease TMPRSS2, which cleaves and activates the spike protein. In the absence of TMPRSS2, endosomal cathepsins can similarly cleave the spike protein. Once activated, the spike protein enables SARS-CoV-2 to fuse with the cellular membrane, releasing its RNA into the cytoplasm to initiate viral replication.
Cellular proteins like Toll-like receptors (TLRs) and IFITM proteins can limit this viral entry by triggering innate immune responses. Evolutionarily, SARS-CoV-2 has developed mutations in its spike protein, such as D614G, which can influence its transmissibility and interaction with the host. These mutations reflect adaptation to humans and potential reservoir species like bats and pangolins, which share genetic homology with the virus. This ongoing adaptability underscores the need for constant genomic surveillance to assess emerging risks and adapt strategies to combat the virus, especially against immune escape mutations in the spike protein that may compromise the efficacy of vaccines and antibody-based therapies. SARS-CoV-2 use the angiotensin-converting enzyme 2 (ACE2) receptor to enter host cells. This receptor is expressed in cardiopulmonary tissues and some hematopoietic cells.
| [14] | Mehta P, McAuley DF, Brown M, Sanchez E, Tattersall RS, Manson JJ. COVID-19: consider cytokine storm syndromes and immunosuppression. The Lancet. 2020; 395(10229): 1033-1034. https://doi.org/10.1016/S0140-6736(20)30628-0 |
| [15] | Zhang C, Wu Z, Li JW, Zhao H, Wang GQ. The cytokine release syndrome (CRS) of severe COVID-19 and interleukin-6 receptor (IL-6R) antagonist Tocilizumab may be the key to reduce the mortality. International Journal of Antimicrobial Agents. 2020; 55(5): 105954. https://doi.org/10.1016/j.ijantimicag.2020.105954 PubMed. |
[14, 15]
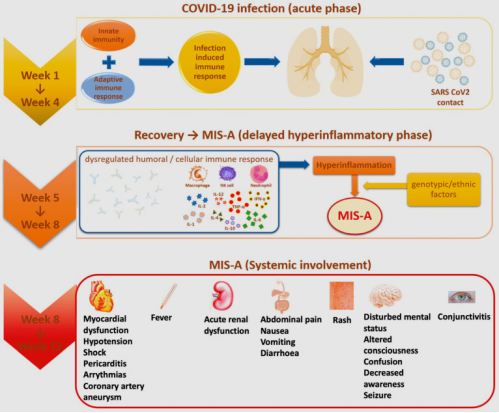
2.6.4. PIMS-TS and SRAS-COV-2
PIMS-TS typically develops weeks after an acute COVID-19 infection, suggesting an immune-mediated mechanism. SARS-CoV-2 infect dendritic cells, leading to apoptosis and depletion of T lymphocytes due to faulty activation caused by dendritic cell dysfunction, contributing to COVID-19 immunopathology.
Clinical features of MIS-C include persistent fever, gastrointestinal symptoms, rash, conjunctivitis, and mucocutaneous inflammation. Cardiac involvement is common, with many children presenting with myocardial dysfunction, elevated cardiac biomarkers, and, in severe cases, shock.
| [21] | Rowley AH. Understanding SARS-CoV-2-related multisystem inflammatory syndrome in children. Nat Rev Immunol. 2020; 20(8): 453-454. https://doi.org/10.1038/s41577-020-0389-2 |
| [33] | Rife, E., Gedalia, A. Maladie de Kawasaki: une mise à jour [Kawasaki disease: an update]. Curr Rheumatol Rep 22, 75 (2020). |
[21, 33]
Laboratory findings often reveal elevated inflammatory markers such as CRP, ferritin, and D-dimer, reflecting the hyperinflammatory state.
A significant feature of severe COVID-19 is cytokine release syndrome, marked by elevated levels of interleukin-6 (IL-6), which correlates with respiratory failure, acute respiratory distress syndrome and adverse clinical outcomes.
High CRP levels, driven by IL-6, are also biomarkers of severe beta-coronavirus infection.
| [33] | Rife, E., Gedalia, A. Maladie de Kawasaki: une mise à jour [Kawasaki disease: an update]. Curr Rheumatol Rep 22, 75 (2020). |
[33]
Infection of monocytes, macrophages and dendritic cells by SARS-CoV-2 leads to their activation and secretion of IL-6 and other inflammatory cytokines, resulting in a "cytokine storm" responsible for a distinctive cardiogenic shock state characterized by vasoplegia and diastolic arterial hypotension.
The management of MIS-C involves a multidisciplinary approach with prompt administration of IVIG and corticosteroids as the mainstay of treatment. Adjunctive therapies such as anakinra or tocilizumab, targeting specific inflammatory pathways, may be used in refractory cases. Supportive care, including fluid resuscitation, inotropic support, and anticoagulation, is critical for managing severe cases with cardiac involvement.
| [1] | Cucinotta D, Vanelli M. WHO Declares COVID-19 a Pandemic. Acta Biomed. 2020 Mar 19; 91(1): 157-160. https://doi.org/10.23750/abm.v91i1.9397 PMID: 32191675; PMCID: PMC7569573. |
| [2] | Moore JB, June CH. Cytokine release syndrome in severe COVID-19. Science. 2020; 368: 473–474. https://doi.org/10.1126/science.abb8925 PMID: 32303591. |
| [33] | Rife, E., Gedalia, A. Maladie de Kawasaki: une mise à jour [Kawasaki disease: an update]. Curr Rheumatol Rep 22, 75 (2020). |
[1, 2, 33]
Figure 1. Pathways leading to cytokine PIMS-TS.
3. Kawasaki Syndrome
Kawasaki syndrome (KS) is characterized by systemic vasculitis primarily affecting medium-sized arteries, particularly the coronary arteries, in children, which can lead to coronary artery aneurysms if not treated promptly.
Kawasaki disease (KD) was first described by Japanese pediatrician Dr. Tomisaku Kawasaki in 1967 in a Japanese-language journal, and later in 1974 in an English-language journal. He observed a 4-year-old boy who exhibited a range of clinical symptoms, including a persistent high-grade fever and a skin rash. Initially, he referred to this condition as “acute febrile mucocutaneous lymph node syndrome” (MCLS). Despite initial skepticism towards the new diagnosis, Dr. Kawasaki remained persistent. After collecting a series of 50 cases, he published his findings, accompanied by meticulous hand-drawn diagrams, in a Japanese medical journal. Dr. Kawasaki outlined the key features of this newly discovered disease, which included persistent fever, bilateral non-purulent conjunctivitis, diffuse oral fissures, a distinctive skin rash, edema of the hands and feet, and lymphadenopathy of the neck.
| [28] | Kawasaki, T. Syndrome cutanéo-muqueux fébrile aigu avec atteinte lymphoïde avec desquamation spécifique des doigts et des orteils chez les enfants [Acute febrile mucocutaneous lymph node syndrome with specific desquamation of the fingers and toes in children]. Arerugi 1967, 16, 178-222. |
[28]
The pathophysiology of Kawasaki syndrome involves a complex interplay of genetic predisposition, immune dysregulation, and potential infectious triggers, although the exact etiology remains elusive. Recent studies have highlighted the role of superantigens and immune complexes in the disease process, contributing to the hyperinflammatory state observed in affected individuals.
According to the American Heart Association (AHA) Guidelines and the Japanese Committee of Kawasaki Disease Research
| [29] | McCrindle, B. W.; Rowley, A. H.; Newburger, J. W.; Burns, J. C.; Bolger, A. F.; Gewitz, M.; Baker, A. L.; Jackson, M. A.; Takahashi, M.; Shah, P. B.; et al. Diagnostic, traitement et gestion à long terme de la maladie de Kawasaki: une déclaration scientifique pour les professionnels de la santé de l’American Heart Association [Diagnosis, treatment, and long-term management of Kawasaki disease: a scientific statement for healthcare professionals from the American Heart Association]. Diffusion 2017, 135, e927-e999. |
| [30] | Ayusawa, M.; Sonobe, T.; Uemura, S.; Ogawa, S.; Nakamura, Y.; Kiyosawa, N.; Ishii, M.; Harada, K. Révision des directives diagnostiques pour la maladie de Kawasaki (la 5e édition révisée) [Revision of diagnostic guidelines for Kawasaki disease (the 5th revised edition)]. Pédiatre int. 2005, 47, 232 à 234. |
| [31] | Gong, G. W.; McCrindle, B. W.; Ching, J. C.; Yeung, R. S. Arthrite se présentant pendant la phase aiguë de la maladie de Kawasaki [Arthritis presenting during the acute phase of Kawasaki disease]. J. Pédiatre. 2006, 148, 800 à 805. |
[29-31]
, there is 5 principal criteria of KD:
1) Strawberry tongue, fissured lips, injected pharynx, and other signs of oropharyngeal mucosa inflammation.
2) Bilateral conjunctivitis (without discharge).
3) Cervical lymph node enlargement of >1.5 cm in diameter of at least one lymph node.
4) Erythema of the palms and soles, edema of the hands and feet in the acute phase, or periungual desquamation after the acute phase.
5) Fever for more than 5 days and a polymorphous skin rash.
Advancements in imaging techniques, particularly echocardiography, have improved the detection and monitoring of coronary artery lesions in KD patients. New biomarkers are also being investigated to aid in early diagnosis and risk stratification.
| [29] | McCrindle, B. W.; Rowley, A. H.; Newburger, J. W.; Burns, J. C.; Bolger, A. F.; Gewitz, M.; Baker, A. L.; Jackson, M. A.; Takahashi, M.; Shah, P. B.; et al. Diagnostic, traitement et gestion à long terme de la maladie de Kawasaki: une déclaration scientifique pour les professionnels de la santé de l’American Heart Association [Diagnosis, treatment, and long-term management of Kawasaki disease: a scientific statement for healthcare professionals from the American Heart Association]. Diffusion 2017, 135, e927-e999. |
| [30] | Ayusawa, M.; Sonobe, T.; Uemura, S.; Ogawa, S.; Nakamura, Y.; Kiyosawa, N.; Ishii, M.; Harada, K. Révision des directives diagnostiques pour la maladie de Kawasaki (la 5e édition révisée) [Revision of diagnostic guidelines for Kawasaki disease (the 5th revised edition)]. Pédiatre int. 2005, 47, 232 à 234. |
| [31] | Gong, G. W.; McCrindle, B. W.; Ching, J. C.; Yeung, R. S. Arthrite se présentant pendant la phase aiguë de la maladie de Kawasaki [Arthritis presenting during the acute phase of Kawasaki disease]. J. Pédiatre. 2006, 148, 800 à 805. |
[29-31]
The treatment for Kawasaki disease (KD) primarily involves high-dose intravenous immunoglobulin (IVIG) and aspirin, which significantly reduce the risk of coronary artery complications. Early administration of IVIG within the first 10 days of illness is crucial for optimal outcomes. In resistant cases, additional treatments such as corticosteroids, infliximab, or cyclosporine may be necessary to control inflammation.
| [29] | McCrindle, B. W.; Rowley, A. H.; Newburger, J. W.; Burns, J. C.; Bolger, A. F.; Gewitz, M.; Baker, A. L.; Jackson, M. A.; Takahashi, M.; Shah, P. B.; et al. Diagnostic, traitement et gestion à long terme de la maladie de Kawasaki: une déclaration scientifique pour les professionnels de la santé de l’American Heart Association [Diagnosis, treatment, and long-term management of Kawasaki disease: a scientific statement for healthcare professionals from the American Heart Association]. Diffusion 2017, 135, e927-e999. |
| [30] | Ayusawa, M.; Sonobe, T.; Uemura, S.; Ogawa, S.; Nakamura, Y.; Kiyosawa, N.; Ishii, M.; Harada, K. Révision des directives diagnostiques pour la maladie de Kawasaki (la 5e édition révisée) [Revision of diagnostic guidelines for Kawasaki disease (the 5th revised edition)]. Pédiatre int. 2005, 47, 232 à 234. |
| [31] | Gong, G. W.; McCrindle, B. W.; Ching, J. C.; Yeung, R. S. Arthrite se présentant pendant la phase aiguë de la maladie de Kawasaki [Arthritis presenting during the acute phase of Kawasaki disease]. J. Pédiatre. 2006, 148, 800 à 805. |
[29-31]
Despite these advancements, ongoing research is essential to fully elucidate the disease mechanisms and improve therapeutic strategies.
3.1. Physiopathology of Kawasaki Syndrome
3.1.1. Immune Activation and Cytokine Release
The initiation of Kawasaki Disease is often hypothesized to involve an infectious trigger, which sets off an exaggerated immune response in genetically susceptible individuals. This immune dysregulation is marked by the activation of T lymphocytes and macrophages within the arterial walls and circulating immune cells. These activated immune cells release a cascade of pro-inflammatory cytokines, including tumor necrosis factor-alpha (TNF-α), interleukin-1 (IL-1), interleukin-6 (IL-6), and interleukin-8 (IL-8). During the acute phase of KD, a "cytokine storm" occurs, characterized by high levels of circulating inflammatory mediators. IL-1, IL-6, and TNF-α play pivotal roles, contributing to systemic inflammation, fever, and endothelial dysfunction. These cytokines drive the widespread inflammation observed in KD and are central to its pathogenesis.
3.1.2. Endothelial Cell Dysfunction
Endothelial cells lining the blood vessels play a critical role in the pathogenesis of Kawasaki Disease. The inflammatory cytokines released during the acute phase of the disease lead to endothelial cell activation and dysfunction. This activation results in increased expression of adhesion molecules such as intercellular adhesion molecule-1 (ICAM-1) and vascular cell adhesion molecule-1 (VCAM-1). These molecules facilitate the recruitment and adhesion of leukocytes to the vascular endothelium, contributing to local inflammation and vascular injury. Activated endothelial cells become dysfunctional, increasing vascular permeability and allowing immune cells to infiltrate the vascular walls. This endothelial activation and subsequent immune cell recruitment lead to further inflammation and damage to the vascular tissue, playing a crucial role in the development of coronary artery aneurysms (CAA).
3.1.3. Formation of Coronary Artery Aneurysms
One of the most serious complications of Kawasaki Disease is the development of coronary artery aneurysms (CAA). The mechanisms underlying CAA formation are multifactorial and likely involve direct vascular injury from inflammatory cells, cytokine-mediated smooth muscle cell proliferation, and impaired endothelial repair mechanisms. Persistent inflammation and ongoing immune activation can further exacerbate vascular remodeling, leading to the dilation and formation of CAA. Matrix metalloproteinases (MMPs), enzymes that degrade the extracellular matrix, are upregulated in KD and contribute to the weakening of the vascular walls. This degradation facilitates the formation of aneurysms, underscoring the importance of controlling inflammation to prevent these severe vascular complications.
3.1.4. Genetic and Environmental Factors
While the exact genetic factors predisposing individuals to Kawasaki Disease are not fully understood, studies suggest a genetic component influencing susceptibility and disease severity. Certain genetic polymorphisms, particularly in genes related to immune regulation and inflammatory responses, may contribute to an exaggerated immune reaction to environmental triggers. Polymorphisms in genes such as ITPKC (inositol 1,4,5-trisphosphate 3-kinase C) and CASP3 (caspase 3) have been associated with an increased risk of developing KD. These genetic variations can influence the intensity and regulation of the immune response, potentially leading to more severe disease manifestations.
| [23] | Kanegaye JT, Wilder MS, Molkara D et al. Recognition of a Kawasaki disease shock syndrome. Pediatrics. 2009; 123: e783-e789. |
| [22] | Mercier, J.-C., Maroni, A. COVID-19 chez l’enfant: syndrome inflammatoire multi-systémique lié à SARS-CoV-2 mimant un syndrome de Kawasaki [COVID-19 in children: multisystem inflammatory syndrome associated with SARS-CoV-2 mimicking Kawasaki syndrome]. |
[23, 22]
3.2. Kawasaki Disease (KD) and Multisystem Inflammatory Syndrome in Children (MIS-C)
COVID-19 has been associated with the emergence of a KD-like condition known as multisystem inflammatory syndrome in children (MIS-C), representing a novel syndrome linked to SARS-CoV-2 infection in pediatric populations.
Kawasaki disease (KD) and Pediatric Inflammatory Multisystem Syndrome Temporally associated with COVID-19 (PIMS-TS) share several key clinical and pathophysiological similarities despite their distinct etiologies. Both conditions primarily affect children, with KD typically seen in younger children under the age of 5 years, while PIMS-TS tends to occur in older children and adolescents following recent or concurrent SARS-CoV-2 infection.
| [34] | Wessels PA, Bingler MA. Une comparaison de la maladie de Kawasaki et du syndrome inflammatoire multisystémique chez les enfants [A comparison of Kawasaki disease and multisystem inflammatory syndrome in children]. Prog Pediatr Cardiol. Juin 2022; 65: 101516. |
[34]
Clinically, both KD and PIMS-TS present with systemic inflammation characterized by prolonged fever, mucocutaneous manifestations (such as rash and conjunctivitis), and systemic involvement that can include cardiovascular, gastrointestinal, and respiratory systems. Elevated inflammatory markers, such as CRP and ferritin, are common in both conditions, reflecting the intense inflammatory response.
| [22] | Mercier, J.-C., Maroni, A. COVID-19 chez l’enfant: syndrome inflammatoire multi-systémique lié à SARS-CoV-2 mimant un syndrome de Kawasaki [COVID-19 in children: multisystem inflammatory syndrome associated with SARS-CoV-2 mimicking Kawasaki syndrome]. |
| [24] | Gámez-González LB, Murata C, Muñoz-Ramírez M, Yamazaki-Nakashimada M Clinical manifestations associated with Kawasaki disease shock syndrome in Mexican children. |
| [34] | Wessels PA, Bingler MA. Une comparaison de la maladie de Kawasaki et du syndrome inflammatoire multisystémique chez les enfants [A comparison of Kawasaki disease and multisystem inflammatory syndrome in children]. Prog Pediatr Cardiol. Juin 2022; 65: 101516. |
[22, 24, 34]
Furthermore, both KD and PIMS-TS can lead to significant cardiovascular complications, including myocarditis and coronary artery abnormalities, although the incidence and severity may vary. Treatment for both conditions often involve immunomodulatory therapies aimed at reducing systemic inflammation and preventing complications, highlighting their shared approach to management despite differences in specific treatment protocols.
| [22] | Mercier, J.-C., Maroni, A. COVID-19 chez l’enfant: syndrome inflammatoire multi-systémique lié à SARS-CoV-2 mimant un syndrome de Kawasaki [COVID-19 in children: multisystem inflammatory syndrome associated with SARS-CoV-2 mimicking Kawasaki syndrome]. |
| [24] | Gámez-González LB, Murata C, Muñoz-Ramírez M, Yamazaki-Nakashimada M Clinical manifestations associated with Kawasaki disease shock syndrome in Mexican children. |
| [32] | Kuo, H.-C. Diagnosis, Progress, and Treatment Update of Kawasaki Disease. Int. J. Mol. Sci. 2023, 24, 13948. https://doi.org/10.3390/ijms241813948 |
| [34] | Wessels PA, Bingler MA. Une comparaison de la maladie de Kawasaki et du syndrome inflammatoire multisystémique chez les enfants [A comparison of Kawasaki disease and multisystem inflammatory syndrome in children]. Prog Pediatr Cardiol. Juin 2022; 65: 101516. |
[22, 24, 32, 34]
Pathophysiologically, while KD's exact cause remains unclear, both KD and PIMS-TS involve dysregulated immune responses triggered by infectious agents, with PIMS-TS specifically linked temporally to SARS-CoV-2 infection. This association underscores the role of viral-triggered immune dysregulation in both conditions, contributing to their overlapping clinical presentations and systemic manifestations.
| [34] | Wessels PA, Bingler MA. Une comparaison de la maladie de Kawasaki et du syndrome inflammatoire multisystémique chez les enfants [A comparison of Kawasaki disease and multisystem inflammatory syndrome in children]. Prog Pediatr Cardiol. Juin 2022; 65: 101516. |
[34]
6. Discussion
The diagnostic criteria established by the American Heart Association categorize Kawasaki-like syndrome into two distinct forms: the complete form, characterized by a high fever lasting at least 5 days and the presence of at least four of the five principal specific clinical signs. Conversely, the incomplete form is characterized by an unexplained fever lasting 5 days or more, accompanied by two to three of the principal clinical signs, supported by laboratory results or cardiac abnormalities.
| [22] | Mercier, J.-C., Maroni, A. COVID-19 chez l’enfant: syndrome inflammatoire multi-systémique lié à SARS-CoV-2 mimant un syndrome de Kawasaki [COVID-19 in children: multisystem inflammatory syndrome associated with SARS-CoV-2 mimicking Kawasaki syndrome]. |
[22]
Post-SARS-CoV-2 PIMS-TS (Pediatric Inflammatory Multisystem Syndrome Temporally associated with SARS-CoV-2) or Kawasaki-like syndrome is defined as complete or incomplete Kawasaki syndrome complicated by hemodynamic instability, necessitating intensive care.
| [24] | Gámez-González LB, Murata C, Muñoz-Ramírez M, Yamazaki-Nakashimada M Clinical manifestations associated with Kawasaki disease shock syndrome in Mexican children. |
[24]
The initial reports of a multisystem inflammatory syndrome affecting children emerged from the United Kingdom, Spain, and New York in April 2020.
| [36] | Feldstein LR, Rose EB, Horwitz SM, et al. Multisystem Inflammatory Syndrome in U.S. Children and Adolescents. New England Journal of Medicine. 2020; 383(4): 334-346. |
[36]
In the following weeks, Italian pediatric rheumatologists observed a significant rise in Kawasaki disease (KD) cases in Italy. Upon evaluation, these cases were similar to Kawasaki disease but occurred in an older pediatric population.
| [38] | Verdoni L, Mazza A, Gervasoni A, et al. An outbreak of severe Kawasaki-like disease at the Italian epicentre of the SARS-CoV-2 epidemic: an observational cohort study. The Lancet. 2020; 395(10239): 1771-1778. |
[38]
There were evident similarities between KD and these MIS-C (Multisystem Inflammatory Syndrome in Children) cases. Some patients developed hemodynamic shock resembling Kawasaki shock syndrome. However, more pronounced differences were noted between these extreme presentations of Kawasaki shock and MIS-C shock.
| [39] | Riphagen S, Gomez X, Gonzalez-Martinez C, et al. Hyperinflammatory shock in children during COVID-19 pandemic. The Lancet. 2020; 395(10237): 1607-1608. |
[39]
Laboratory abnormalities in MIS-C shock cases were significantly more pronounced compared to Kawasaki shock. Both groups exhibited elevated CRP and ferritin levels, but these elevations were less pronounced in Kawasaki disease shock.
| [36] | Feldstein LR, Rose EB, Horwitz SM, et al. Multisystem Inflammatory Syndrome in U.S. Children and Adolescents. New England Journal of Medicine. 2020; 383(4): 334-346. |
[36]
Additionally, the ethnic background of patients differed, with MIS-C patients predominantly being African American/Hispanic, while Kawasaki disease patients who developed shock were more often of Asian descent.
| [40] | Toubiana J, Poirault C, Corsia A, et al. Kawasaki-like multisystem inflammatory syndrome in children during the covid-19 pandemic in Paris, France: prospective observational study. BMJ. 2020; 369. |
[40]
Distinct differences included lymphopenia, low platelet count, and low albumin levels in COVID-19 patients, whereas Kawasaki shock patients did not develop lymphopenia, had less severe thrombocytopenia that reversed within 10 to 14 days and transformed into prolonged thrombocytosis.
In MIS-C patients, platelet counts normalized after the acute phase. The most distinct clinical feature of MIS-C compared to Kawasaki was significant myocardial dysfunction with elevated troponin and BNP markers. In contrast, coronary artery involvement and secondary cardiac dysfunction were predominant in severe Kawasaki cases, with slightly elevated BNP and troponin levels.
To identify differences in immune activation between MIS-C and Kawasaki disease, Consiglio et al. conducted an analysis of immune cell systems, cytokines, and antibodies in patients with Kawasaki disease, MIS-C, SARS-CoV-2 infection, and healthy children.
| [35] | Consiglio CR, Cotugno N, Sardh F, et al. The Immunology of Multisystem Inflammatory Syndrome in Children with COVID-19. Nature Medicine. 2020; 26(10): 1664-1670. |
[35]
Their primary analysis revealed that MIS-C overlapped to some extent with Kawasaki hyperimmune syndrome and adult hyperimmune syndrome post-COVID-19.
However, most cytokine profiles were distinct across these subgroups. Principal component analysis showed more similarities in cytokine profiles between MIS-C and SARS-CoV-2 infected children, differing from Kawasaki patients.
Notable differences included IL-6, IL-17, CXCL10, ADA, and SCF. In Kawasaki disease, IL-6, IL-17, and CXCL10 were uniformly expressed at higher levels than in MIS-C and SARS-CoV-2 positive patients. However, between MIS-C and SARS-CoV-2 positive patients, levels were more heterogeneous, suggesting a spectrum rather than two distinct diseases.
| [40] | Toubiana J, Poirault C, Corsia A, et al. Kawasaki-like multisystem inflammatory syndrome in children during the covid-19 pandemic in Paris, France: prospective observational study. BMJ. 2020; 369. |
[40]
Most importantly, the proteome profiling study indicated the presence of immunity against known coronaviruses (human coronavirus 1 and bovine beta coronavirus) in healthy children, SARS-CoV-2 infected patients, and Kawasaki patients, which was surprisingly negative in all MIS-C cohorts.
| [35] | Consiglio CR, Cotugno N, Sardh F, et al. The Immunology of Multisystem Inflammatory Syndrome in Children with COVID-19. Nature Medicine. 2020; 26(10): 1664-1670. |
[35]
Before discussing the implications of this finding and relevant immune activation pathways related to coronavirus infections, it would be safer to replicate these data in larger series.
The study also found Endoglin antibodies in both MIS-C and Kawasaki patients, indicating endothelial and cardiac muscle damage. However, MAP2K2 and casein kinase family members were exclusively found in MIS-C. Silmitasertib (CX-4945), a potent antiviral known to inhibit these kinases, is suggested for adjunctive treatment in COVID-19 patients and is currently in clinical trials. Additionally, Kawasaki patients showed more plasma markers of arterial damage than MIS-C, with specific antibodies playing roles in vascular wall regeneration and angiogenesis, highlighting distinct pathogenic mechanisms.
| [42] | Ramaswamy A, Brodsky NN, Sumida TS, et al. Immune dysregulation and autoreactivity in autoimmune myocarditis induced by checkpoint inhibitors. Cancer Discovery. 2021; 11(4): 891-908. |
[42]
Only 15% of MIS-C patients met KD criteria, emphasizing distinct clinical and immunological profiles between the two conditions. Efforts to identify gene activations during Kawasaki and MIS-C revealed overlapping pathways but distinct transcriptional signatures, providing further insights into the unique pathophysiology of MIS-C and pediatric COVID-19.
| [41] | Cheung EW, Zachariah P, Gorelik M, et al. Multisystem inflammatory syndrome related to COVID-19 in previously healthy children and adolescents in New York City. JAMA. 2020; 324(3): 294-296. |
[41]
In summary, proteomic analysis suggests that while there is overlap, MIS-C and Kawasaki disease involve different pathway activations, targeted structural anomalies, and distinct markers of damage such as endothelial versus myocardial involvement. International data from a large series of MIS-C patients indicated a more severe presentation with higher BNP, D-dimer, CRP, and ferritin levels, and greater cardiac complications compared to Kawasaki patients.
| [37] | Whittaker E, Bamford A, Kenny J, et al. Clinical Characteristics of 58 Children With a Pediatric Inflammatory Multisystem Syndrome Temporally Associated With SARS-CoV-2. JAMA. 2020; 324(3): 259-269. |
[37]
The results of our study align with previous findings that also identified an overlap between the diagnostic criteria for Kawasaki syndrome and MIS-C post-COVID 19. syndrome
| [25] | Lin Y-J, Cheng M-C, Lo M-H, Chien S-J Early differentiation of Kawasaki disease shock syndrome and toxic shock syndrome in a pediatric intensive care unit. Pediatr Infect Dis J. 2015; 34: 1163-1167. |
| [26] | Gamez-Gonzalez LB, Moribe-Quintero I, Cisneros-Castolo M, et al. Kawasaki disease shock syndrome: unique and severe subtype of Kawasaki disease. |
| [27] | Fernández-Sarmiento J, De Souza D, Jabornisky R, Gonzalez GA, Arias López MDP, Palacio G. Paediatric inflammatory multisystem syndrome temporally associated with COVID-19 (PIMS-TS): a narrative review and the viewpoint of the Latin American Society of Pediatric Intensive Care (SLACIP) Sepsis Committee. BMJ Paediatr Open. 2021 Feb 4; 5(1): e000894. https://doi.org/10.1136/bmjpo-2020-000894 PMID: 34192188; PMCID: PMC7868133. |
[25-27]