A brain abscess is defined as an encapsulated lesion of the central nervous system. It is an infrequent occurrence, particularly in the pediatric population with no relevant history. There are multiple routes of infection, but in pediatrics, inoculation by contiguity or hematogenous infection under specific conditions predominates. We present the clinical case of an 8-year-old male patient with no relevant personal or family history. The patient presented with a nonspecific clinical picture of intermittent headaches that had been evolving for 2 months. There were no ostensible neurological alterations. A normal physical examination was conducted on admission. However, a giant brain abscess in the frontal lobe was identified by brain computed tomography. The only potential cause that could be identified was an odontogenic origin. The patient was approached by the neurosurgery team, who proceeded to empty the abscess capsule. A brain secretion culture was also conducted, which yielded isolation of Streptococcus viridans. It is established that this etiological agent is of very low virulence and rarely produces symptoms in immunocompetent patients, representing a low disease burden. However, in the event of infection, it can have severe repercussions. It is noteworthy that the patient did not present positive acute phase reactants, no positive blood tests, and no other relevant findings were evidenced despite the large mass effect and edema evidenced in the neuroimages taken.
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited.
A brain abscess is a rare infection of the central nervous system, defined by the presence of a localized collection of pus resulting from an infectious process. The estimated incidence of this condition is 0.4 to 0.9 cases per 100,000 inhabitants per year. It is more prevalent in men and typically affects children under the age of 15, with a peak incidence between the ages of 4 and 7. And increases the prevalence to 2 to 3 cases per 10,000 hospitalized patients. A predisposing factor is immunocompromised patients or patients with valvular heart disease
[1]
Brouwer MC, Tunkel AR, McKhann GM 2nd, van de Beek D. Brain abscess. N Engl J Med [Internet]. 2014; 371(5): 447–56. Available:
Christopher J. Harrison RB. Focal Suppurative Infections of the Nervous System. En: Drs. Sarah S. Long, Charles G. Prober, Marc Fischer, editor. Principles and Practice of Pediatric Infectious Diseases. Elsevier; 2022. p. 46, 337-347. e3.
[3]
Handbook of Clinical Neurology. Vol. 112 (3er series). Pediatric Neurology Part II. O. Dulac, M. Lassonde, and HB Sarnat, Editors. 2013. Elsevier.
[1-3]
. In approximately 50% of cases, the abscess is located in the superficial frontal region
[4]
Pérez-Cárdenas SH, Márquez-Herrera KC, Echeverría-Palacio CM, Cárdenas-Hernández VC, Parrado-Sánchez ZD, Bustos-Acosta JC. Factores asociados al pronóstico de morbimortalidad en pacientes pediátricos con absceso cerebral. Infectio [Internet]. 2024; 27-32. Available:
The route of inoculation can be contiguous (40%), for example, in the context of sinusitis, otitis, or mastoiditis, trauma, surgery, or hematogenous (30%), in the context of pulmonary diseases or of unknown source. A variety of etiologic agents have been identified, with Streptococcus bacteria accounting for approximately 36% of cases and the Viridans subspecies representing less than 6%. There has been a notable reduction in mortality rates over time, with the current rate estimated to be approximately 20%.
Streptococcus viridans is a gram-positive bacterium of low virulence that resides in the normal bacterial flora of the oral mucosa. It rarely produces infectious clinical manifestations; however, it is expected to predominantly affect immunocompromised patients and develop life-threatening diseases
[1]
Brouwer MC, Tunkel AR, McKhann GM 2nd, van de Beek D. Brain abscess. N Engl J Med [Internet]. 2014; 371(5): 447–56. Available:
Christopher J. Harrison RB. Focal Suppurative Infections of the Nervous System. En: Drs. Sarah S. Long, Charles G. Prober, Marc Fischer, editor. Principles and Practice of Pediatric Infectious Diseases. Elsevier; 2022. p. 46, 337-347. e3.
[4]
Pérez-Cárdenas SH, Márquez-Herrera KC, Echeverría-Palacio CM, Cárdenas-Hernández VC, Parrado-Sánchez ZD, Bustos-Acosta JC. Factores asociados al pronóstico de morbimortalidad en pacientes pediátricos con absceso cerebral. Infectio [Internet]. 2024; 27-32. Available:
MD y Peter J. Hotez, Ralph D. Feigin JDC, editor. Feigin and Cherry’s Textbook of Pediatric Infectious Diseases. Filadelfia, PA, Estados Unidos de América: Saunders; 2009. p. 84, 835-856. e7.
[1, 2, 4-6]
.
In the meta-analysis conducted by doctor Brouwer and colleagues, cerebral abscesses with potential odontogenic entry represent only 5% of the total cases studied
[7]
Brouwer MC, Coutinho JM, van de Beek D. Clinical characteristics and outcome of brain abscess: systematic review and meta-analysis. Neurology [Internet]. 2014; 82(9): 806–13. Available:
. This clinical case presents a male patient of 8 years of age with no previous history of significance. The patient presents with a nonspecific condition of 2 months' duration and persistent severe headache, despite outpatient management. Neuroimaging reveals an important collection in the right frontal lobe, necessitating neurosurgery. Additionally, an odontogenic etiology is identified, though the findings remain inconclusive regarding the lesion's evolution, causal agent, and extent.
2. Case Description
This is an 8-year-old male patient with a clinical history of 2 months' duration, characterized by intermittent holocranial headaches of moderate to severe intensity, with no other associations. He was initially seen on an outpatient basis, where he was treated with non-steroidal anti-inflammatory drugs and evaluated by the optometry team, who detected a visual refraction disorder. Consequently, they recommended the use of prescription glasses, although this did not result in any improvement in the headaches.
One month prior to his admission, the patient presented with left palpebral edema, an unquantified febrile sensation, and an alteration in the mobility of the ipsilateral eyeball. There was no evidence of conjunctival injection or purulent secretion. The patient was managed with acetaminophen and a first-generation cephalosporin, with complete resolution of the picture observed on the third day. Two weeks later, the patient reported an intensification of the headache, accompanied by episodes of emesis of gastric contents and nocturnal awakenings due to pain. This prompted a consultation with the emergency department.
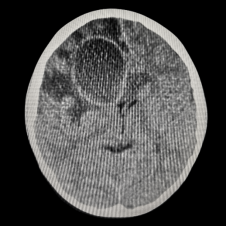
The physical examination yielded no significant findings. The patient was afebrile, exhibited adequate vital signs, and demonstrated normal anthropometric parameters for her sex and age. Laboratory tests were conducted, including a complete blood count, prothrombin time, C-reactive protein (CRP) level, and procalcitonin level. These tests yielded results within the normal range and negative acute phase reactants. However, due to the persistence of the headache, a brain CT scan was recommended. This imaging procedure revealed a well-defined hypodense lesion in the right frontal lobe. The lesion was 52x77x44 mm in size and was associated with extensive vasogenic edema, midline deviation, and compression of the ipsilateral lateral ventricle (Figure 1). Additionally, there were no alterations observed in the sinuses for paranasal sinuses, mastoid cells, and periocular fat. Empirical antibiotic therapy was initiated with Cefepime, Vancomycin, and Metronidazole after blood cultures were obtained and incubated for five days, which yielded negative results.
Figure 1. Simple axial computed tomography of the skull showed a well-defined hypodense lesion in the right frontal lobe, with diameters of 52x77x44 mm, associated with extensive vasogenic edema, midline deviation and compression of the ipsilateral lateral ventricle. There were no lesions visible in the bone window.
The patient was subsequently taken to craniotomy by the neurosurgery team, who performed drainage of 60 ml of purulent material and sent it to culture. Streptococcus viridans was isolated. Targeted antibiotic therapy with penicillin was adjusted.
The patient was evaluated by a pediatric cardiologist, who performed an echocardiogram and found normal biventricular function, no pathological findings or vegetations, and no abnormalities in the ophthalmology evaluation. However, the dental team found dental caries with pulp necrosis of tooth number 75 and root debris of tooth number 85, indicating the need for exodontia. The patient exhibited a satisfactory clinical evolution, without evidence of neurological alterations. Additionally, serological tests for HIV, infections by germs of the TORCHS group, and immunological tests were conducted, all of which yielded results within the normal range.
3. Discussion
A brain abscess is an uncommon infection with multiple potential etiologies. It presents as a circumscribed, encapsulated lesion in the cerebral parenchyma, resulting from a fibroblast-mediated reaction that secretes alpha actin of smooth muscle, forming a capsule with perilesional edema. This occurs subsequent to an inflammatory process caused by cerebritis, leading to cytotoxic edema and subsequent necrosis. A variety of routes of inoculation and causative agents have been identified. However, in pediatric patients, the condition occurs under specific conditions, such as trauma, local infection in neighboring sites (e.g., otitis, sinusitis, mastoiditis, etc.), alterations of cardiac valves, and immunosuppression
[1]
Brouwer MC, Tunkel AR, McKhann GM 2nd, van de Beek D. Brain abscess. N Engl J Med [Internet]. 2014; 371(5): 447–56. Available:
Diana Catalina Gómez-Muñoz MD, Darwin Raúl Lara-Botina MD, Adriana Páez MD, Luis Gabriel Vinasco. Absceso cerebral: una entidad poco común en pediatría. Revista ecuatoriana de neuro. 2024; 33(2).
The clinical manifestations are typically nonspecific and dependent on the location and mass effect. Commonly, focal or systemic neurological symptoms (between 50% and 70%) are observed, accompanied by fever (60%), vomiting (47%), headache (70%), and seizures (62.5%). The suspicion is confirmed. Neuroimaging studies, such as CT scans or positron magnetic resonance imaging of the brain (the gold standard for differentiating abscesses from tumors or metastases), reveal unspecific blood biochemistry in the majority of cases. However, it is estimated that 80% of patients exhibit elevated acute phase reactants.
[4]
Pérez-Cárdenas SH, Márquez-Herrera KC, Echeverría-Palacio CM, Cárdenas-Hernández VC, Parrado-Sánchez ZD, Bustos-Acosta JC. Factores asociados al pronóstico de morbimortalidad en pacientes pediátricos con absceso cerebral. Infectio [Internet]. 2024; 27-32. Available:
Brouwer MC, Coutinho JM, van de Beek D. Clinical characteristics and outcome of brain abscess: systematic review and meta-analysis. Neurology [Internet]. 2014; 82(9): 806–13. Available:
Gallego C, Autero C, Pérez M, Meningitis D. Absceso cerebral. Encefalitis aguda. Protoc diagn ter pediatr. Sociedad española de infectologia pediátrica. 2023; 2: 309–28.
[10]
Raffaldi I, Garazzino S, Castelli G. Brain abscesses in children: an Italian multicentre study. Epidemiol. Infect. 2017.
Sáez-Llorens, Xavier; Nieto-Guevara, Javier. Brain abscess. Chapter 116. Handbook of Clinical Neurology, Vol 112 (3d series) Pediatric Neurology Part II. Elsevier. 2013.
[12]
Diana Catalina Gómez-Muñoz MD, Darwin Raúl Lara-Botina MD, Adriana Páez MD, Luis Gabriel Vinasco. Absceso cerebral: una entidad poco común en pediatría. Revista ecuatoriana de neuro. 2024; 33(2).
Brizuela M, Pérez G, Martiren S, et al. Absceso cerebral en niños: experiencia en diez años en un hospital pediátrico de alta complejidad. Arch Argent Pediatr. 2017; 115(04): 230-232.
. The sensitivity of cultures is typically 80% or higher, and in-hospital stays in the intensive care unit are anticipated in approximately 40% of cases, with an average length of stay of approximately 3 days
[7]
Brouwer MC, Coutinho JM, van de Beek D. Clinical characteristics and outcome of brain abscess: systematic review and meta-analysis. Neurology [Internet]. 2014; 82(9): 806–13. Available:
Gallego C, Autero C, Pérez M, Meningitis D. Absceso cerebral. Encefalitis aguda. Protoc diagn ter pediatr. Sociedad española de infectologia pediátrica. 2023; 2: 309–28.
[9]
Andrew B. Janowski DAH. Brain Abscess. En: St. Geme RK&. JW III, editor. Nelson Textbook of Pediatrics. Elsevier; 2024. p. Chapter 644, 3779-3781. e1.
[7-9]
.
In a study conducted in Colombia by Pérez-Cardenas and colleagues, the most prevalent causative agents in pediatrics were Streptococcus aureus and Streptococcus pneumonia
[4]
Pérez-Cárdenas SH, Márquez-Herrera KC, Echeverría-Palacio CM, Cárdenas-Hernández VC, Parrado-Sánchez ZD, Bustos-Acosta JC. Factores asociados al pronóstico de morbimortalidad en pacientes pediátricos con absceso cerebral. Infectio [Internet]. 2024; 27-32. Available:
The Streptococcus viridans family is a Gram-positive, catalase-negative, α-hemolytic bacterial genus with low virulence. It is a fundamental component of the normal bacterial flora of the oral mucosa
[6]
MD y Peter J. Hotez, Ralph D. Feigin JDC, editor. Feigin and Cherry’s Textbook of Pediatric Infectious Diseases. Filadelfia, PA, Estados Unidos de América: Saunders; 2009. p. 84, 835-856. e7.
[14]
Laulajainen-Hongisto A, Lempinen L, Färkkilä E, Saat R, Markkola A, Leskinen K, et al. Intracranial abscesses over the last four decades; changes in etio-logy, diagnostics, treatment and outcome. Infect Dis (Lond). 2016; 48: 310-316.
Heine AC, García S, Barberis C, Vay C, E Mollerach M, Bonofiglio L, et al. Identificación y sensibilidad a los antimicrobianos de aislados de estreptococos del grupo viridans provenientes de pacientes internados en un hospital universitario de la ciudad de Buenos Aires. Rev Argent Microbiol [Internet]. 2019; 51(1): 26–31. Disponible en:
. As they are not large pathogens, they commonly invade only surrounding tissues in conditions of transient immunosuppression, penetrating trauma, or gingival alterations. However, in 37% of cases, bacteremia, endocarditis, and septic emboli can occur when performing dental procedures, particularly in immunosuppressed states (especially neutropenia) and/or heart valve diseases up to 40-60% of cases.
[6]
MD y Peter J. Hotez, Ralph D. Feigin JDC, editor. Feigin and Cherry’s Textbook of Pediatric Infectious Diseases. Filadelfia, PA, Estados Unidos de América: Saunders; 2009. p. 84, 835-856. e7.
[7]
Brouwer MC, Coutinho JM, van de Beek D. Clinical characteristics and outcome of brain abscess: systematic review and meta-analysis. Neurology [Internet]. 2014; 82(9): 806–13. Available:
Laulajainen-Hongisto A, Lempinen L, Färkkilä E, Saat R, Markkola A, Leskinen K, et al. Intracranial abscesses over the last four decades; changes in etio-logy, diagnostics, treatment and outcome. Infect Dis (Lond). 2016; 48: 310-316.
. Fortunately, the microorganism is largely susceptible to penicillin, contingent on its affinity to bind to penicillin-binding proteins. However, recent evidence suggests that up to 20% of cases exhibit resistance to this treatment, particularly in instances of endocarditis. Consequently, third-generation cephalosporins and carbapenemics are currently regarded as the preferred treatment option in in vitro studies
[16]
Lopardo HA, Vigliarolo L, Bonofiglio L, Gagetti P, García Gabarrot G, Kaufman S, et al. Beta-lactam antibiotics and viridans group streptococci. Rev Argent Microbiol [Internet]. 2022; 54(4): 335–43. Disponible en:
The present clinical case is noteworthy for several reasons. First, the patient had no significant personal history. Second, the etiological agent represents less than 6% of cases in the pediatric population. Third, the clinical presentation, although typical for headache and vomiting, it was not relevantly remarkable, particularly in the absence of a febrile syndrome, which would be expected to raise diagnostic suspicion. It’s unusual that the patient did not present any other neurological manifestations despite the extent of the lesion. Additionally, the patient did not exhibit the typical clinical behavior, as evidenced by the absence of acute phase reactants elevation and leukocytosis, which are observed in more than 70% of cases.
Abbreviations
CPR
C-protein Reactive
mm
Millimeters
ml
Milliliters
HIV
Human Immunodeficiency Virus
TORCHS
Toxoplasmosis, Rubella Cytomegalovirus, Herpes Simplex, HIV and Syphilis
CT scan
Computed Tomography
Ethical Responsibilities
An informed consent form has been completed and signed by the legal representative (mother), and the research committee of the institution where the clinical history was taken has granted authorization, thereby ensuring the patient's right to privacy and guaranteeing the protection of his or her identity in accordance with international regulations.
Economic Financing
No financial support was received.
Author Contributions
Juan Sebastian Pimienta Parra: Writing – original draft
José Manuel Carrera Sánchez: Supervision
Conflicts of Interest
The authors declare no conflicts of interest.
References
[1]
Brouwer MC, Tunkel AR, McKhann GM 2nd, van de Beek D. Brain abscess. N Engl J Med [Internet]. 2014; 371(5): 447–56. Available:
Christopher J. Harrison RB. Focal Suppurative Infections of the Nervous System. En: Drs. Sarah S. Long, Charles G. Prober, Marc Fischer, editor. Principles and Practice of Pediatric Infectious Diseases. Elsevier; 2022. p. 46, 337-347. e3.
[3]
Handbook of Clinical Neurology. Vol. 112 (3er series). Pediatric Neurology Part II. O. Dulac, M. Lassonde, and HB Sarnat, Editors. 2013. Elsevier.
[4]
Pérez-Cárdenas SH, Márquez-Herrera KC, Echeverría-Palacio CM, Cárdenas-Hernández VC, Parrado-Sánchez ZD, Bustos-Acosta JC. Factores asociados al pronóstico de morbimortalidad en pacientes pediátricos con absceso cerebral. Infectio [Internet]. 2024; 27-32. Available:
MD y Peter J. Hotez, Ralph D. Feigin JDC, editor. Feigin and Cherry’s Textbook of Pediatric Infectious Diseases. Filadelfia, PA, Estados Unidos de América: Saunders; 2009. p. 84, 835-856. e7.
[7]
Brouwer MC, Coutinho JM, van de Beek D. Clinical characteristics and outcome of brain abscess: systematic review and meta-analysis. Neurology [Internet]. 2014; 82(9): 806–13. Available:
Gallego C, Autero C, Pérez M, Meningitis D. Absceso cerebral. Encefalitis aguda. Protoc diagn ter pediatr. Sociedad española de infectologia pediátrica. 2023; 2: 309–28.
[9]
Andrew B. Janowski DAH. Brain Abscess. En: St. Geme RK&. JW III, editor. Nelson Textbook of Pediatrics. Elsevier; 2024. p. Chapter 644, 3779-3781. e1.
[10]
Raffaldi I, Garazzino S, Castelli G. Brain abscesses in children: an Italian multicentre study. Epidemiol. Infect. 2017.
Sáez-Llorens, Xavier; Nieto-Guevara, Javier. Brain abscess. Chapter 116. Handbook of Clinical Neurology, Vol 112 (3d series) Pediatric Neurology Part II. Elsevier. 2013.
[12]
Diana Catalina Gómez-Muñoz MD, Darwin Raúl Lara-Botina MD, Adriana Páez MD, Luis Gabriel Vinasco. Absceso cerebral: una entidad poco común en pediatría. Revista ecuatoriana de neuro. 2024; 33(2).
Brizuela M, Pérez G, Martiren S, et al. Absceso cerebral en niños: experiencia en diez años en un hospital pediátrico de alta complejidad. Arch Argent Pediatr. 2017; 115(04): 230-232.
Laulajainen-Hongisto A, Lempinen L, Färkkilä E, Saat R, Markkola A, Leskinen K, et al. Intracranial abscesses over the last four decades; changes in etio-logy, diagnostics, treatment and outcome. Infect Dis (Lond). 2016; 48: 310-316.
Heine AC, García S, Barberis C, Vay C, E Mollerach M, Bonofiglio L, et al. Identificación y sensibilidad a los antimicrobianos de aislados de estreptococos del grupo viridans provenientes de pacientes internados en un hospital universitario de la ciudad de Buenos Aires. Rev Argent Microbiol [Internet]. 2019; 51(1): 26–31. Disponible en:
Parra, J. S. P., Sánchez, J. M. C. (2024). Giant Frontal Brain Abscess Due to Streptococcus Viridans in an 8-Year-Old Patient: Case Report. American Journal of Pediatrics, 10(4), 240-243. https://doi.org/10.11648/j.ajp.20241004.23
Parra, J. S. P.; Sánchez, J. M. C. Giant Frontal Brain Abscess Due to Streptococcus Viridans in an 8-Year-Old Patient: Case Report. Am. J. Pediatr.2024, 10(4), 240-243. doi: 10.11648/j.ajp.20241004.23
Parra JSP, Sánchez JMC. Giant Frontal Brain Abscess Due to Streptococcus Viridans in an 8-Year-Old Patient: Case Report. Am J Pediatr. 2024;10(4):240-243. doi: 10.11648/j.ajp.20241004.23
@article{10.11648/j.ajp.20241004.23,
author = {Juan Sebastian Pimienta Parra and José Manuel Carrera Sánchez},
title = {Giant Frontal Brain Abscess Due to Streptococcus Viridans in an 8-Year-Old Patient: Case Report},
journal = {American Journal of Pediatrics},
volume = {10},
number = {4},
pages = {240-243},
doi = {10.11648/j.ajp.20241004.23},
url = {https://doi.org/10.11648/j.ajp.20241004.23},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ajp.20241004.23},
abstract = {A brain abscess is defined as an encapsulated lesion of the central nervous system. It is an infrequent occurrence, particularly in the pediatric population with no relevant history. There are multiple routes of infection, but in pediatrics, inoculation by contiguity or hematogenous infection under specific conditions predominates. We present the clinical case of an 8-year-old male patient with no relevant personal or family history. The patient presented with a nonspecific clinical picture of intermittent headaches that had been evolving for 2 months. There were no ostensible neurological alterations. A normal physical examination was conducted on admission. However, a giant brain abscess in the frontal lobe was identified by brain computed tomography. The only potential cause that could be identified was an odontogenic origin. The patient was approached by the neurosurgery team, who proceeded to empty the abscess capsule. A brain secretion culture was also conducted, which yielded isolation of Streptococcus viridans. It is established that this etiological agent is of very low virulence and rarely produces symptoms in immunocompetent patients, representing a low disease burden. However, in the event of infection, it can have severe repercussions. It is noteworthy that the patient did not present positive acute phase reactants, no positive blood tests, and no other relevant findings were evidenced despite the large mass effect and edema evidenced in the neuroimages taken.},
year = {2024}
}
TY - JOUR
T1 - Giant Frontal Brain Abscess Due to Streptococcus Viridans in an 8-Year-Old Patient: Case Report
AU - Juan Sebastian Pimienta Parra
AU - José Manuel Carrera Sánchez
Y1 - 2024/12/30
PY - 2024
N1 - https://doi.org/10.11648/j.ajp.20241004.23
DO - 10.11648/j.ajp.20241004.23
T2 - American Journal of Pediatrics
JF - American Journal of Pediatrics
JO - American Journal of Pediatrics
SP - 240
EP - 243
PB - Science Publishing Group
SN - 2472-0909
UR - https://doi.org/10.11648/j.ajp.20241004.23
AB - A brain abscess is defined as an encapsulated lesion of the central nervous system. It is an infrequent occurrence, particularly in the pediatric population with no relevant history. There are multiple routes of infection, but in pediatrics, inoculation by contiguity or hematogenous infection under specific conditions predominates. We present the clinical case of an 8-year-old male patient with no relevant personal or family history. The patient presented with a nonspecific clinical picture of intermittent headaches that had been evolving for 2 months. There were no ostensible neurological alterations. A normal physical examination was conducted on admission. However, a giant brain abscess in the frontal lobe was identified by brain computed tomography. The only potential cause that could be identified was an odontogenic origin. The patient was approached by the neurosurgery team, who proceeded to empty the abscess capsule. A brain secretion culture was also conducted, which yielded isolation of Streptococcus viridans. It is established that this etiological agent is of very low virulence and rarely produces symptoms in immunocompetent patients, representing a low disease burden. However, in the event of infection, it can have severe repercussions. It is noteworthy that the patient did not present positive acute phase reactants, no positive blood tests, and no other relevant findings were evidenced despite the large mass effect and edema evidenced in the neuroimages taken.
VL - 10
IS - 4
ER -
Parra, J. S. P., Sánchez, J. M. C. (2024). Giant Frontal Brain Abscess Due to Streptococcus Viridans in an 8-Year-Old Patient: Case Report. American Journal of Pediatrics, 10(4), 240-243. https://doi.org/10.11648/j.ajp.20241004.23
Parra, J. S. P.; Sánchez, J. M. C. Giant Frontal Brain Abscess Due to Streptococcus Viridans in an 8-Year-Old Patient: Case Report. Am. J. Pediatr.2024, 10(4), 240-243. doi: 10.11648/j.ajp.20241004.23
Parra JSP, Sánchez JMC. Giant Frontal Brain Abscess Due to Streptococcus Viridans in an 8-Year-Old Patient: Case Report. Am J Pediatr. 2024;10(4):240-243. doi: 10.11648/j.ajp.20241004.23
@article{10.11648/j.ajp.20241004.23,
author = {Juan Sebastian Pimienta Parra and José Manuel Carrera Sánchez},
title = {Giant Frontal Brain Abscess Due to Streptococcus Viridans in an 8-Year-Old Patient: Case Report},
journal = {American Journal of Pediatrics},
volume = {10},
number = {4},
pages = {240-243},
doi = {10.11648/j.ajp.20241004.23},
url = {https://doi.org/10.11648/j.ajp.20241004.23},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ajp.20241004.23},
abstract = {A brain abscess is defined as an encapsulated lesion of the central nervous system. It is an infrequent occurrence, particularly in the pediatric population with no relevant history. There are multiple routes of infection, but in pediatrics, inoculation by contiguity or hematogenous infection under specific conditions predominates. We present the clinical case of an 8-year-old male patient with no relevant personal or family history. The patient presented with a nonspecific clinical picture of intermittent headaches that had been evolving for 2 months. There were no ostensible neurological alterations. A normal physical examination was conducted on admission. However, a giant brain abscess in the frontal lobe was identified by brain computed tomography. The only potential cause that could be identified was an odontogenic origin. The patient was approached by the neurosurgery team, who proceeded to empty the abscess capsule. A brain secretion culture was also conducted, which yielded isolation of Streptococcus viridans. It is established that this etiological agent is of very low virulence and rarely produces symptoms in immunocompetent patients, representing a low disease burden. However, in the event of infection, it can have severe repercussions. It is noteworthy that the patient did not present positive acute phase reactants, no positive blood tests, and no other relevant findings were evidenced despite the large mass effect and edema evidenced in the neuroimages taken.},
year = {2024}
}
TY - JOUR
T1 - Giant Frontal Brain Abscess Due to Streptococcus Viridans in an 8-Year-Old Patient: Case Report
AU - Juan Sebastian Pimienta Parra
AU - José Manuel Carrera Sánchez
Y1 - 2024/12/30
PY - 2024
N1 - https://doi.org/10.11648/j.ajp.20241004.23
DO - 10.11648/j.ajp.20241004.23
T2 - American Journal of Pediatrics
JF - American Journal of Pediatrics
JO - American Journal of Pediatrics
SP - 240
EP - 243
PB - Science Publishing Group
SN - 2472-0909
UR - https://doi.org/10.11648/j.ajp.20241004.23
AB - A brain abscess is defined as an encapsulated lesion of the central nervous system. It is an infrequent occurrence, particularly in the pediatric population with no relevant history. There are multiple routes of infection, but in pediatrics, inoculation by contiguity or hematogenous infection under specific conditions predominates. We present the clinical case of an 8-year-old male patient with no relevant personal or family history. The patient presented with a nonspecific clinical picture of intermittent headaches that had been evolving for 2 months. There were no ostensible neurological alterations. A normal physical examination was conducted on admission. However, a giant brain abscess in the frontal lobe was identified by brain computed tomography. The only potential cause that could be identified was an odontogenic origin. The patient was approached by the neurosurgery team, who proceeded to empty the abscess capsule. A brain secretion culture was also conducted, which yielded isolation of Streptococcus viridans. It is established that this etiological agent is of very low virulence and rarely produces symptoms in immunocompetent patients, representing a low disease burden. However, in the event of infection, it can have severe repercussions. It is noteworthy that the patient did not present positive acute phase reactants, no positive blood tests, and no other relevant findings were evidenced despite the large mass effect and edema evidenced in the neuroimages taken.
VL - 10
IS - 4
ER -