Multiple pregnancies with more than two fetuses significantly increase maternal and infant complications. Almost all multiple pregnancies with more than two fetuses result in preterm birth. Prematurity is the main consequence of multiple pregnancies with more than two fetuses. Early provision of optimal nutrition is crucial for the growth and immunity of premature infants. We report our first-hand experience as the primary referral hospital in West Nusa Tenggara Province, Indonesia, in providing multidisciplinary care for the birth of quadruplet premature infants. A 39-year-old woman, gravida 3, para 2, living 2, nulliparous, was referred to the General Hospital of West Nusa Tenggara Province from Bima District Hospital due to a quadruplet pregnancy at 28-29 weeks gestation. A multidisciplinary team consisting of obstetricians, pediatricians, and nurses was assembled. All four infants were diagnosed with hyaline membrane disease (HMD) and immediately transferred to the Neonatal Intensive Care Unit (NICU). Premature infants received parenteral and enteral nutrition support. Family-centered care approach was implemented for the care of the premature infants and their families. All infants were discharged at 35 weeks postmenstrual age (PMA). Spontaneous quadruplet pregnancies are rare cases, and this particular case represents the first experience of our hospital in managing quadruplet infants. A well-coordinated multidisciplinary approach, coupled with good preparedness for delivery, is essential and has proven to yield favorable outcomes for both the mother and the infants.
| Published in | American Journal of Pediatrics (Volume 10, Issue 4) |
| DOI | 10.11648/j.ajp.20241004.20 |
| Page(s) | 220-228 |
| Creative Commons |
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited. |
| Copyright |
Copyright © The Author(s), 2024. Published by Science Publishing Group |
Quadruplet Pregnancy, Quadriplet, Premature Infant Management
Quadruplet | G | BW | BL | HC | MUAC | APGAR | TOB |
|---|---|---|---|---|---|---|---|
First | Male | 1350 | 39 | 27 | 6,5 | 5-7 | 08.30 |
Second | Male | 1370 | 40 | 27 | 6,5 | 3-5 | 08.31 |
Third | Male | 1100 | 37 | 26 | 6 | 5-7 | 08.32 |
fourth | Male | 1195 | 37 | 28 | 6 | 5-7 | 08.33 |
PMA | First | Second | Third | Fourth |
|---|---|---|---|---|
29 + 0 | 1350 | 1370 | 1100 | 1195 |
29 + 5 | 1270 | 1235 | 1090 | 1164 |
30 + 6 | 1510 | 1530 | 1200 | 1350 |
31 + 5 | 1640 | 1603 | 1260 | 1508 |
32 + 2 | 1835 | 1660 | 1400 | 1671 |
32 + 5 | 1930 | 1800 | 1560 | 1772 |
32 + 6 | 2000 | 1930 | 1630 | 1800 |
33 + 1 | 2030 | 2070 | 1706 | 1820 |
33 + 2 | 2055 | 2095 | 1723 | 1850 |
33 + 5 | 2150 | 2150 | 1730 | 1930 |
33 + 6 | 2180 | 2175 | 1760 | 1955 |
34 + 0 | 2230 | 2220 | 1785 | 1995 |
34 + 2 | 2360 | 2290 | 1790 | 2030 |
34 + 6 | 2375 | 2305 | 1800 | 2095 |
35 + 5 | 2800 | 2660 | 1965 | 2180 |
HMD | Hyaline Membrane Disease |
PMA | Postmenstrual Age |
G | Gender |
MUAC | Mid Upper Arm Circumference (cm) |
BW | Body Weight (gram) |
APGAR | APGAR Scores at 1’, 5’ |
BL | Body Length (cm) |
TOB | Time of Birth |
HC | Head Circumference (cm) |
PEEP | Positive End Expiratory Pressure |
MAP | Mean Airway Pressure |
| [1] | Umeora OUJ, Aneziokoro EA, Egwuatu VE. Higher-order multiple births in Abakaliki, Southeast Nigeria. Vol. 52, Singapore Medical Journal. 2011. |
| [2] | Shrestha D, Thapa B, Aryal S, Shrestha BK, Kalakheti B, Panthee K. Successful Management of Quadruplet Pregnancy following Spontaneous Conception. J Lumbini Med Coll. 2016; 4(1). |
| [3] | Goldman GA, Dicker D, Peleg D, Goldman JA. Is Elective Cerclage Justified in the Management of Triplet and Quadruplet Pregnancy? Aust New Zeal J Obstet Gynaecol. 1989; 29(1). |
| [4] | Mansouri HA, Ghazawi AH. The maternal and neonatal outcome of high order gestation at King Abdulaziz University Hospital. Vol. 275, Archives of Gynecology and Obstetrics. 2007. |
| [5] | Bronstein JM. The Population Dimension: The Distribution of Preterm Births. In: Preterm Birth in the United States. 2016. |
| [6] | Shih-Ching L, Hsing-Chun L, and Cheau-Feng L. Nutritional Care of Preterm Infants: from Global Guidelines to Local Practice. Asian Journal of Dietetics. 2020. |
| [7] | Barr S, Poggi S, Keszler M. Triplet morbidity and mortality in a large case series. J Perinatol. 2003; 23(5). |
| [8] | Nnadi D, Nwobodo E, Ibrahim A. Spontaneous monochorionic tetra-amniotic quadruplet pregnancy at term. J Basic Clin Reprod Sci. 2013; 2(1). |
| [9] | Ng EH, Shah V. Guidelines for surfactant replacement therapy in neonates. Paediatr Child Heal. 2021; 26(1). |
| [10] | Liu Y, Wang XT, Li HY, Hou HY, Wang H, Wang YT. Safety and Efficacy of Higher Order Multifetal Pregnancy Reduction: A Single-Center Retrospective Study. Vol. 10, AJP Reports. 2020. |
| [11] | Kaoutar Khabbache et al. Current respiratory support practices in premature infants: an observational study. Pan African Medical Journal. 2021; 39(66). |
| [12] | Minuye Birihane B, Alebachew Bayih W, Yeshambel Alemu A, Belay DM, Demis A. The burden of hyaline membrane disease, mortality and its determinant factors among preterm neonates admitted at Debre Tabor General Hospital, North Central Ethiopia: A retrospective follow up study. PLoS One. 2021; 16(3). |
| [13] | Hiles M, Culpan AM, Watts C, Munyombwe T, Wolstenhulme S. Neonatal respiratory distress syndrome: Chest X-ray or lung ultrasound? A systematic review. Vol. 25, Ultrasound. 2017. |
| [14] | Dyer J. Neonatal respiratory distress syndrome: Tackling a worldwide problem. Vol. 44, P and T. 2019. |
| [15] | Tochie JN, Choukem SP, Langmia RN, Barla E, Ndombo PK. Neonatal respiratory distress in a reference neonatal unit in Cameroon: An analysis of prevalence, predictors, etiologies and outcomes. Pan Afr Med J. 2016; 24. |
| [16] | Pang H, Zhang B, Shi J, Zang J, Qiu L. Diagnostic value of lung ultrasound in evaluating the severity of neonatal respiratory distress syndrome. Eur J Radiol. 2019; 116. |
| [17] | Sabol BA, Caughey AB. Acidemia in neonates with a 5-minute Apgar score of 7 or greater – What are the outcomes? In: American Journal of Obstetrics and Gynecology. 2016. |
| [18] | Iliodromiti S, MacKay DF, Smith GCS, Pell JP, Nelson SM. Apgar score and the risk of cause-specific infant mortality: A population-based cohort study. Lancet. 2014; 384(9956). |
| [19] | Polin RA, Carlo WA. Surfactant Replacement Therapy for Preterm and Term Neonates With Respiratory Distress. In: Neonatal Care: A Compendium of AAP Clinical Practice Guidelines and Policies. 2021. |
| [20] | Plavka R, Kopecký P, Sebroň V, Leiská A, Švihovec P, Ruffer J, et al. Early versus delayed surfactant administration in extremely premature neonates with respiratory distress syndrome ventilated by high-frequency oscillatory ventilation. Intensive Care Med. 2002; 28(10). |
| [21] | Hay WW. Nutritional support strategies for the preterm infant in the neonatal intensive care unit. Vol. 21, Pediatric Gastroenterology, Hepatology and Nutrition. 2018. |
| [22] | Binenbaum G, Bell EF, Donohue P, Quinn G, Shaffer J, Tomlinson LA, et al. Development of modified screening criteria for retinopathy of prematurity primary results from the postnatal growth and retinopathy of prematurity study. In: JAMA Ophthalmology. 2018. |
| [23] | WHO recommendations for care of the preterm or low-birth-weight infant. Geneva: World Health Organization. 2022; Licence: CC BY-NC-SA 3.0 IGO. |
| [24] | Morgan AS., Mendonca M., Rhiele N., and David AL. Management and outcomes of extreme preterm birth. BMJ 2022; 376: e055924. |
| [25] | Medise BE. Growth and Development in Preterm Infants: What is The Long-Term Risk?. Amerta Nutr. 2021; supl. 27-33. |
| [26] | Belfort MB, Gillman MW, Buka SL, Casey PH, McCormick MC. Preterm Infant Linear Growth and Adiposity Gain: Trade-Offs for Later Weight Status and Intelligence Quotient. J Pediatr. 2013; 163(6). |
| [27] | Belfort MB, Rifas-Shiman SL, Sullivan T, Collins CT, McPhee AJ, Ryan P, et al. Infant growth before and after term: Effects on neurodevelopment in preterm infants. Pediatrics. 2011; 128(4). |
| [28] | Rosenbaum P, King S, Law M, King G, Evans J. Family-centred service: A conceptual framework and research review. Vol. 18, Physical and Occupational Therapy in Pediatrics. 1998. |
| [29] | Yu YT, Hsieh WS, Hsu CH, Lin YJ, Lin CH, Hsieh S, et al. Family-centered care improved neonatal medical and neurobehavioral outcomes in preterm infants: Randomized controlled trial. Phys Ther. 2017; 97(12). |
| [30] | Symington AJ, Pinelli J. Developmental care for promoting development and preventing morbidity in preterm infants. Vol. 2009, Cochrane Database of Systematic Reviews. 2006. |
APA Style
Indrasuari, L. M., Wirawan, I. K. A., Hamid, A. R. H. (2024). Management of Quadruplet Infants at the General Hospital of West Nusa Tenggara Province, Indonesia: A Case Report. American Journal of Pediatrics, 10(4), 220-228. https://doi.org/10.11648/j.ajp.20241004.20
ACS Style
Indrasuari, L. M.; Wirawan, I. K. A.; Hamid, A. R. H. Management of Quadruplet Infants at the General Hospital of West Nusa Tenggara Province, Indonesia: A Case Report. Am. J. Pediatr. 2024, 10(4), 220-228. doi: 10.11648/j.ajp.20241004.20
AMA Style
Indrasuari LM, Wirawan IKA, Hamid ARH. Management of Quadruplet Infants at the General Hospital of West Nusa Tenggara Province, Indonesia: A Case Report. Am J Pediatr. 2024;10(4):220-228. doi: 10.11648/j.ajp.20241004.20
@article{10.11648/j.ajp.20241004.20,
author = {Luh Made Indrasuari and I Ketut Adi Wirawan and Agus Rusdhy Hariawan Hamid},
title = {Management of Quadruplet Infants at the General Hospital of West Nusa Tenggara Province, Indonesia: A Case Report
},
journal = {American Journal of Pediatrics},
volume = {10},
number = {4},
pages = {220-228},
doi = {10.11648/j.ajp.20241004.20},
url = {https://doi.org/10.11648/j.ajp.20241004.20},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ajp.20241004.20},
abstract = {Multiple pregnancies with more than two fetuses significantly increase maternal and infant complications. Almost all multiple pregnancies with more than two fetuses result in preterm birth. Prematurity is the main consequence of multiple pregnancies with more than two fetuses. Early provision of optimal nutrition is crucial for the growth and immunity of premature infants. We report our first-hand experience as the primary referral hospital in West Nusa Tenggara Province, Indonesia, in providing multidisciplinary care for the birth of quadruplet premature infants. A 39-year-old woman, gravida 3, para 2, living 2, nulliparous, was referred to the General Hospital of West Nusa Tenggara Province from Bima District Hospital due to a quadruplet pregnancy at 28-29 weeks gestation. A multidisciplinary team consisting of obstetricians, pediatricians, and nurses was assembled. All four infants were diagnosed with hyaline membrane disease (HMD) and immediately transferred to the Neonatal Intensive Care Unit (NICU). Premature infants received parenteral and enteral nutrition support. Family-centered care approach was implemented for the care of the premature infants and their families. All infants were discharged at 35 weeks postmenstrual age (PMA). Spontaneous quadruplet pregnancies are rare cases, and this particular case represents the first experience of our hospital in managing quadruplet infants. A well-coordinated multidisciplinary approach, coupled with good preparedness for delivery, is essential and has proven to yield favorable outcomes for both the mother and the infants.
},
year = {2024}
}
TY - JOUR T1 - Management of Quadruplet Infants at the General Hospital of West Nusa Tenggara Province, Indonesia: A Case Report AU - Luh Made Indrasuari AU - I Ketut Adi Wirawan AU - Agus Rusdhy Hariawan Hamid Y1 - 2024/12/16 PY - 2024 N1 - https://doi.org/10.11648/j.ajp.20241004.20 DO - 10.11648/j.ajp.20241004.20 T2 - American Journal of Pediatrics JF - American Journal of Pediatrics JO - American Journal of Pediatrics SP - 220 EP - 228 PB - Science Publishing Group SN - 2472-0909 UR - https://doi.org/10.11648/j.ajp.20241004.20 AB - Multiple pregnancies with more than two fetuses significantly increase maternal and infant complications. Almost all multiple pregnancies with more than two fetuses result in preterm birth. Prematurity is the main consequence of multiple pregnancies with more than two fetuses. Early provision of optimal nutrition is crucial for the growth and immunity of premature infants. We report our first-hand experience as the primary referral hospital in West Nusa Tenggara Province, Indonesia, in providing multidisciplinary care for the birth of quadruplet premature infants. A 39-year-old woman, gravida 3, para 2, living 2, nulliparous, was referred to the General Hospital of West Nusa Tenggara Province from Bima District Hospital due to a quadruplet pregnancy at 28-29 weeks gestation. A multidisciplinary team consisting of obstetricians, pediatricians, and nurses was assembled. All four infants were diagnosed with hyaline membrane disease (HMD) and immediately transferred to the Neonatal Intensive Care Unit (NICU). Premature infants received parenteral and enteral nutrition support. Family-centered care approach was implemented for the care of the premature infants and their families. All infants were discharged at 35 weeks postmenstrual age (PMA). Spontaneous quadruplet pregnancies are rare cases, and this particular case represents the first experience of our hospital in managing quadruplet infants. A well-coordinated multidisciplinary approach, coupled with good preparedness for delivery, is essential and has proven to yield favorable outcomes for both the mother and the infants. VL - 10 IS - 4 ER -
Department of Child Health, West Nusa Tenggara Province General Hospital, Medical Faculty of Mataram University, Mataram, Indonesia

Figure 1. The prepared resuscitation team in managing quadruplet infants at the Regional General Hospital of West Nusa Tenggara Province (NTB) engaging in prayer before proceeding with the cesarean section procedure.

Figure 2. Pediatric specialist and team during the neonatal resuscitation process for the fourth infants.
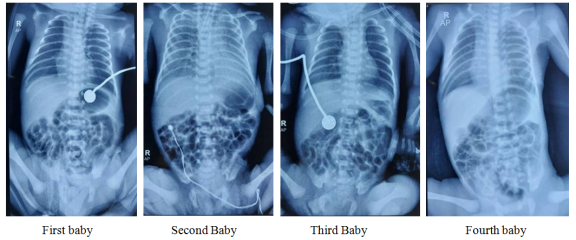
Figure 3. Thoraco-abdominal X-ray image of the quadruplet babies showing features of Hyaline Membrane Disease (HMD).
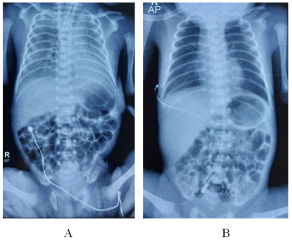
Figure 4. A. Thoraco-abdominal X-ray of the second baby shows inadequate lung expansion due to grade III HMD. B. Thoraco-abdominal X-ray of the second baby after surfactant therapy demonstrates improved lung expansion in both lung lobes.
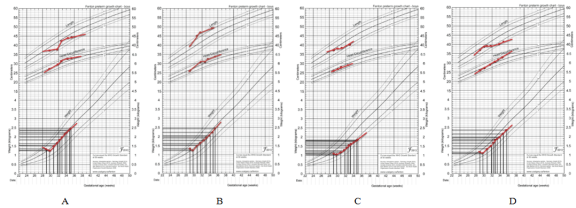
Figure 5. Fenton Premature Growth Chart for Premature Infants, A. First Baby, B. Second Baby, C. Third Baby, D. Fourth Baby.

Figure 6. Kangaroo mother care for premature babies.

Figure 7. Family-Centered Care implemented for premature infants in our hospital.

Figure 8. The quadruplets and mother returning home in a healthy condition.

