Miliary TB is one of the manifestations of TB with incidence 3-7% among all TB cases and 13% can spread to brain as Tuberculous Meningitis (TBM). This case report discusses a case of miliary TB complicated with meningoencephalitis in children under two years of age without history of BCG vaccination. A 23-month-old girl with severe malnutrition, came to outpatient clinic with fever for 6 months, cough for 3 months, gland enlargement in the neck, no history of BCG and no history of TB contact. Because the chest x-ray showed miliary TB, we decided to hospitalized the patient. Suddenly she had loss of consciousness and seizures in the way to pediatric ward. After being managed and stabilized, we decided do head CT scan with contrast and found multiple rim enhancing lesions, with a smooth inner outer layer. Mycobacterium Tuberculosis was detected without rifampicin resistance by Polymerase Chain Reaction (PCR) TB from sputum speciment, but not detected in liquor cerebro spinal (LCS). Cerebrospinal fluid analysis showed mononuclear cell dominant (87%). The patient was given broad spectrum antibiotic, anti-seizures drug, and intensive phase anti-tuberculosis drugs with RHZE and steroid. The patient was discharged with clinical improvement after 3 weeks of treatment but had sequelae of cerebral palsy. Early detection and appropriate management are crucial in pediatric patients with miliary TB to reduce mortality rate and prevent TBM, which can lead to permanent neurological disabilities.
| Published in | American Journal of Pediatrics (Volume 10, Issue 4) |
| DOI | 10.11648/j.ajp.20241004.21 |
| Page(s) | 229-233 |
| Creative Commons |
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited. |
| Copyright |
Copyright © The Author(s), 2024. Published by Science Publishing Group |
Miliary TB, Tuberculous Meningitis, Children
TB | Tuberculosis |
TBM | Tuberculous Meningitis |
BCG vaccine | Bacille Calmette-Guérin Vaccine |
GCS | Glasgow Coma Scale |
| [1] | Utami, D. A., Purniti, N. P. S., Subanada, I. B. & MM, A. S. Faktor Risiko Infeksi Tuberkulosis Milier dan Ekstraparu pada Anak Penderita Tuberkulosis. Sari Pediatr. 22, (2021). |
| [2] | Sharma, S. K., Mohan, A. & Sharma, A. Challenges in the diagnosis & treatment of miliary tuberculosis. Indian Journal of Medical Research vol. 135 (2012). |
| [3] | Magdalena, C. C., Utomo, B. & Setyoningrum, R. A. Risk factors for miliary tuberculosis in children. Paediatr. Indones. 57, (2017). |
| [4] | Blount, R. J. T. et al. Childhood Tuberculosis in Northern Viet Nam: A Review of 103 Cases. Plos One vol. 9, (2014). |
| [5] | Wu, X. R. et al. Pediatric tuberculosis at Beijing Children’s Hospital: 2002-2010. Pediatrics 130, (2012). |
| [6] | Daniel, B., Grace, G. & Natrajan, M. Tuberculous meningitis in children: Clinical management & outcome. Indian Journal of Medical Research vol. 150(2019). |
| [7] | Chiang, S. S. et al. Treatment outcomes of childhood tuberculous meningitis: A systematic review and meta-analysis. Lancet Infect. Dis. 14, (2014). |
| [8] | Israni, A. V. et al. Tubercular meningitis in children: Clinical, pathological, and radiological profile and factors associated with mortality. J. Neurosci. Rural Pract. 7, (2016). |
| [9] | Duc, L. A. et al. Miliary brain tuberculosis in an infant. Radiol. Case Reports 16, (2021). |
| [10] | Kanesen, D. et al. Clinical outcome of tuberculous meningitis with hydrocephalus — a retrospective study. Malaysian J. Med. Sci. 28, (2021). |
| [11] | Huynh, J. et al. Tuberculous Meningitis in Children: Reducing the Burden of Death and Disability. Pathogens vol. 11 (2022). |
| [12] | Khan, F. Y. Review of literature on disseminated tuberculosis with emphasis on the focused diagnostic workup. Journal of Family and Community Medicine vol. 26 (2019). |
| [13] | Mert, A. et al. Miliary tuberculosis: Epidemiologicaland clinical analysis of large-case series from moderate to low tuberculosis endemic Country. Medicine (Baltimore). 96, (2017). |
| [14] | Mert A, Arslan F, Kuyucu T, et al. Miliary tuberculosis: Epidemiological and clinical analysis of large-case series from moderate to low tuberculosis endemic Country. Medicine (Baltimore). 2017; 96(5): e5875. |
| [15] | Van Toorn, R. & Solomons, R. Update on the diagnosis and management of tuberculous meningitis in children. Semin. Pediatr. Neurol. 21, (2014). |
| [16] | Chatterjee, S. Brain tuberculomas, tubercular meningitis, and post-tubercular hydrocephalus in children. Journal of Pediatric Neurosciences vol. 6 (2011). |
| [17] | Module 5: Management of tuberculosis in children and adolescents-Consolidated Guidelines on Tuberculosis TreatmentWorld Health Organization, (WHO). Module 5: Management of tuberculosis in children and adolescents-Consolidated Guidelines on Tuberculosis TreatmentWorld Health Organization, (WHO). Who (2020). |
| [18] | Rock, R. B., Olin, M., Baker, C. A., Molitor, T. W. & Peterson, P. K. Central nervous system tuberculosis: Pathogenesis and clinical aspects. Clinical Microbiology Reviews vol. 21 (2008). |
| [19] | Cruz, A. T., Garcia-Prats, A. J., Furin, J. & Seddon, J. A. Treatment of multidrug-resistant tuberculosis infection in children. Pediatr. Infect. Dis. J. 37, (2018). |
| [20] | Awaluddin, S. M. et al. Characteristics of paediatric patients with tuberculosis and associated determinants of treatment success in Malaysia using the MyTB version 2.1 database over five years. BMC Public Health 20, (2020). |
| [21] | Van Well, G. T. J. et al. Twenty years of pediatric tuberculous meningitis: A retrospective cohort study in the western cape of south africa. Pediatrics 123, (2009). |
| [22] | Van Den Bos, F. et al. Tuberculous meningitis and miliary tuberculosis in young children. Trop. Med. Int. Heal. 9, (2004). |
| [23] | Cherian, A. & Thomas, S. V. Central nervous system tuberculosis. Afr. Health Sci. 11, (2011). |
| [24] | Gräb, J. et al. Corticosteroids inhibit Mycobacterium tuberculosis-induced necrotic host cell death by abrogating mitochondrial membrane permeability transition. Nat. Commun. 10, (2019). |
| [25] | Ewa AU, Bassey GE, Udoh UA, Akpah EU, Anachuna KC, Ekeng BE. Miliary Tuberculosis with Severe Pneumonia without Abnormal Chest Sounds in a Covid-19 Pandemic. MedDocs Publishers: J Tuberc. 2021; 4(1). 1-4. |
APA Style
Indrasuari, L. M., Indriyani, S. A. K. (2024). Miliary Tuberculosis with Tuberculous Meningoencephalitis in Children Under Two Years of Age with a Missed Opportunity of Immunization: A Case Report. American Journal of Pediatrics, 10(4), 229-233. https://doi.org/10.11648/j.ajp.20241004.21
ACS Style
Indrasuari, L. M.; Indriyani, S. A. K. Miliary Tuberculosis with Tuberculous Meningoencephalitis in Children Under Two Years of Age with a Missed Opportunity of Immunization: A Case Report. Am. J. Pediatr. 2024, 10(4), 229-233. doi: 10.11648/j.ajp.20241004.21
AMA Style
Indrasuari LM, Indriyani SAK. Miliary Tuberculosis with Tuberculous Meningoencephalitis in Children Under Two Years of Age with a Missed Opportunity of Immunization: A Case Report. Am J Pediatr. 2024;10(4):229-233. doi: 10.11648/j.ajp.20241004.21
@article{10.11648/j.ajp.20241004.21,
author = {Luh Made Indrasuari and Sang Ayu Kompiyang Indriyani},
title = {Miliary Tuberculosis with Tuberculous Meningoencephalitis in Children Under Two Years of Age with a Missed Opportunity of Immunization: A Case Report
},
journal = {American Journal of Pediatrics},
volume = {10},
number = {4},
pages = {229-233},
doi = {10.11648/j.ajp.20241004.21},
url = {https://doi.org/10.11648/j.ajp.20241004.21},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ajp.20241004.21},
abstract = {Miliary TB is one of the manifestations of TB with incidence 3-7% among all TB cases and 13% can spread to brain as Tuberculous Meningitis (TBM). This case report discusses a case of miliary TB complicated with meningoencephalitis in children under two years of age without history of BCG vaccination. A 23-month-old girl with severe malnutrition, came to outpatient clinic with fever for 6 months, cough for 3 months, gland enlargement in the neck, no history of BCG and no history of TB contact. Because the chest x-ray showed miliary TB, we decided to hospitalized the patient. Suddenly she had loss of consciousness and seizures in the way to pediatric ward. After being managed and stabilized, we decided do head CT scan with contrast and found multiple rim enhancing lesions, with a smooth inner outer layer. Mycobacterium Tuberculosis was detected without rifampicin resistance by Polymerase Chain Reaction (PCR) TB from sputum speciment, but not detected in liquor cerebro spinal (LCS). Cerebrospinal fluid analysis showed mononuclear cell dominant (87%). The patient was given broad spectrum antibiotic, anti-seizures drug, and intensive phase anti-tuberculosis drugs with RHZE and steroid. The patient was discharged with clinical improvement after 3 weeks of treatment but had sequelae of cerebral palsy. Early detection and appropriate management are crucial in pediatric patients with miliary TB to reduce mortality rate and prevent TBM, which can lead to permanent neurological disabilities.
},
year = {2024}
}
TY - JOUR T1 - Miliary Tuberculosis with Tuberculous Meningoencephalitis in Children Under Two Years of Age with a Missed Opportunity of Immunization: A Case Report AU - Luh Made Indrasuari AU - Sang Ayu Kompiyang Indriyani Y1 - 2024/12/16 PY - 2024 N1 - https://doi.org/10.11648/j.ajp.20241004.21 DO - 10.11648/j.ajp.20241004.21 T2 - American Journal of Pediatrics JF - American Journal of Pediatrics JO - American Journal of Pediatrics SP - 229 EP - 233 PB - Science Publishing Group SN - 2472-0909 UR - https://doi.org/10.11648/j.ajp.20241004.21 AB - Miliary TB is one of the manifestations of TB with incidence 3-7% among all TB cases and 13% can spread to brain as Tuberculous Meningitis (TBM). This case report discusses a case of miliary TB complicated with meningoencephalitis in children under two years of age without history of BCG vaccination. A 23-month-old girl with severe malnutrition, came to outpatient clinic with fever for 6 months, cough for 3 months, gland enlargement in the neck, no history of BCG and no history of TB contact. Because the chest x-ray showed miliary TB, we decided to hospitalized the patient. Suddenly she had loss of consciousness and seizures in the way to pediatric ward. After being managed and stabilized, we decided do head CT scan with contrast and found multiple rim enhancing lesions, with a smooth inner outer layer. Mycobacterium Tuberculosis was detected without rifampicin resistance by Polymerase Chain Reaction (PCR) TB from sputum speciment, but not detected in liquor cerebro spinal (LCS). Cerebrospinal fluid analysis showed mononuclear cell dominant (87%). The patient was given broad spectrum antibiotic, anti-seizures drug, and intensive phase anti-tuberculosis drugs with RHZE and steroid. The patient was discharged with clinical improvement after 3 weeks of treatment but had sequelae of cerebral palsy. Early detection and appropriate management are crucial in pediatric patients with miliary TB to reduce mortality rate and prevent TBM, which can lead to permanent neurological disabilities. VL - 10 IS - 4 ER -
Department of Child Health, West Nusa Tenggara Province General Hospital, Medical Faculty of Mataram University, Mataram, Indonesia
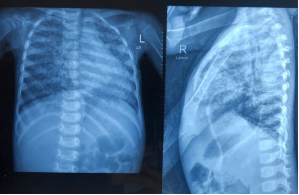
Figure 1. Anteroposterior (AP) and lateral chest X-ray images showing infiltrates consistent with the appearance of miliary tuberculosis (TB) in both lung fields.
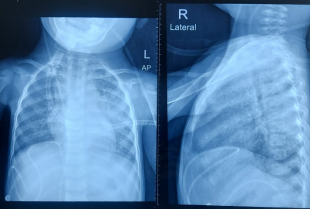
Figure 2. Evaluation of anteroposterior (AP) and lateral chest X-ray images after three weeks of therapy.
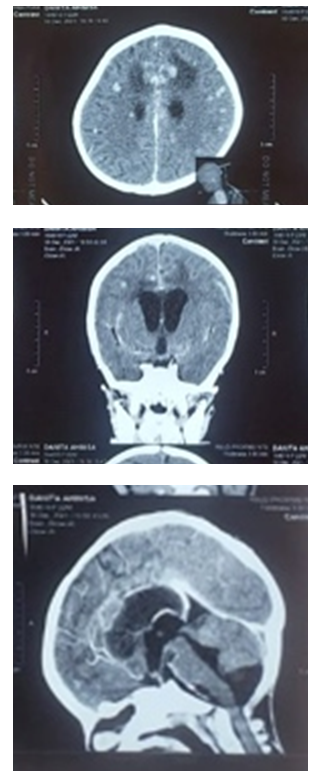
Figure 3. Head CT scan showing multiple rim-enhancing lesions with smooth inner and outer layers suggestive of tuberculous meningitis.
Information

